

【中西合璧】针灸治疗女性纤维肌痛的随机对照试验:中医辨证下取穴群体针灸



上海中医药大学附属龙华医院麻醉科

目的:比较群体针灸与群体教育对纤维肌痛患者的治疗效果。
方法:选取确诊为纤维肌痛(美国放射学会 1990 年标准),中度至重度疼痛水平的女性30名,随机分成两组,分别进行群体针灸或群体教育治疗10周(共 900分钟)。每周评估FIQR总量、疼痛VAS评分,并在基线、5周和10周、治疗结束后随访4周后评估全球疲劳指数。
结果:针灸组患者平均治疗时间为810分钟,教育组患者平均治疗时间为 861分钟。针灸组在FIQR 总量、疼痛和全球疲劳指数在治疗结束时和治疗后4周与治疗前对比有显著差异,但在群体组中则没有变化。
结论:与群体教育相比,群体针灸有效缓解了患者FIQR总量、疼痛和疲劳指数。
关键词:纤维肌痛、群针、中医、疼痛、疲劳、随机对照试验
背景:纤维肌痛是一种多症状疾病,其特点是慢性广泛性疼痛,伴随疲劳、睡眠等全身问题,严重者甚至发生认知障碍、抑郁和焦虑 [1] [2]。在美国约有400万患者 [3],而且此疾病容易被没有缺乏经验的医生误诊[4]。纤维肌痛占用了大量的医疗资源,并影响患者的正常工作,对社会造成极大的经济损失[5,6]。
许多纤维肌痛患者,诸如许多慢性疼痛患者一样,除了常规使用药物治疗以外,仍然会选择其他一种药物替代方案。据估计,近40%的人尝试过至少一种药物替代方案[7]。同一份报告表明,近7%的人使用过针灸治疗。在纤维肌痛治疗指南文件中,建议对纤维肌痛患者进行思想教育疏导[8],而对针灸治疗持保留态度。
相当多的研究文献表明针灸效果参差不齐。最近Lauche 等人 [9]发现针灸可能对治疗纤维肌痛有效。然而在另外两篇文献中,没有足够证据证明针灸治疗有效。 [10,11],在所有可以查到的综述中,还没有研究过群体针灸治疗纤维肌痛患者。
在本研究中,我们报告了群体针灸与群体教育的两组治疗纤维肌痛患者的临床试验的结果。该研究评估群体针灸治疗纤维肌痛患者的有效性和可行性,并且结果提示群体针灸对药物治疗无效女性仍然有一定的效果。
患者和方法
本研究按照 1990 年美国放射学会定义的诊断标准,选取18-75岁纤维肌痛的女性患者,视觉模拟量表 (VAS) 平均疼痛为5以上(包括5),并同意在研究期间不更改任何药物或治疗方案,同时这些患者贝克抑郁量表评分低于29分[ 17] 以及在过去六个月内未使用过针灸或东方医学的人。排除麻醉剂或有药物滥用史、怀孕或哺乳期妇女、患有凝血功能或自身免疫性疾病患者以及正在接受残疾鉴定或参与与纤维肌痛相关的诉讼的人。此外,他们必须进行中医辨证,包括肝气郁结、气血郁结或气血两虚。
在这项研究中,使用最小似然分配法将参与者随机分配成两组,针灸组和教育组[ 18-20],针灸组进行10周的群体针灸,教育组进行10周的群体教育,并在治疗后随访1个月。分配程序通过权衡随机化来确定分组,以消除两组在关键特征上的差异。分配基线测量值包括纤维肌痛影响问卷评分、针灸治疗预期(您期望组针灸能在多大程度上改善您的纤维肌痛症状?0表示没有变化,7表示不再出现症状)、体重指数 (BMI)和年龄。在获得基线测量值后,参与者会被告知分配在哪一个组。
干预措施
群体针灸,也称为社区针灸,该组患者每周接受两次群体针灸治疗,采用中医辨证取穴,每次针灸持续约40分钟。中医辨证包括传统的脉象和舌诊以及和患者深入的访谈。实施者在该领域有丰富的临床经验,并且在研究开始前参加校准练习 [ 15 , 21]。针灸治疗在一个设有八张针灸台的房间内进行。患者可以互相交谈,但一旦针头到位,他们往往会安静地休息。每次治疗仅限于25 根针(Tempo 品牌 0.16 毫米 × 40 毫米或 0.20 毫米 × 40 毫米)。如果需要,针灸师可以手动操作针头。在选取针灸师时要求要求针灸师有至少五年的诊疗经验,但实际上所有针灸师都有超过10年的诊疗经验。
中医辨证取穴
a、 以中医证候为基础
一、脾湿:CV12、CV9、ST28、ST36、SP9、SP6、KD7、BL22
二、痰瘀:ST36、SP9、神关、SP6、KD3、KD7、ST44、LV3、SP4、CV6、CV4
三、气滞:GB34、LV3、TB6、LI4
四、血瘀:BL17、SP10、PC6、KD14(SP4、PC6合在一起)
五、 寒痹:ST36,SP9,神关,SP7。SP6,KD3,KD7,CV4,CV6
六、SP气虚:ST36、SP3、CV12、CV6
七、脾阳虚证:BL20、BL23、KD7、CV4、CV6
八、肾气虚证:ST36、SP3、CV12、CV6、KD3
九、肾阳虚:BL20、BL23、KD7、CV4、CV6
十、 肝血虚:LV8、KD3、CV4、SP6
十一、肝阴虚证:LV8、KD3、CV4、SP6
十二、肾阴虚证:LV8、KD3、CV4、SP6
十三、心血虚:HT7、ST36、SP6、LV8、CV4
b、 根据症状:
一、 头痛:GV20、LI4、太阳、GB41、ST41、SJ5。
二、失眠:HT7或P6,SP6,安眠。
三.抑郁和/或焦虑:GV24、GV20、CV17、CV15、CV12、CV6、印堂。
如果出现其他症状,医生将同时治疗主要症状和其他症状
群体教育是一个便利的教育过程。该组的参与者就纤维肌痛书籍中的章节进行小组讨论,讨论重点是当前对纤维肌痛病因、人口统计学以及药物和非药物治疗方案的理解 [21]。在讨论中,各参与者积极发言。选择群体教育作为对照的原因是,在教育过程中,参与者都可以参与,融入讨论,它既考虑了群体针灸中医师与患者的互动,也考虑了总治疗时间。
数据收集
研究的主要数据结果是纤维肌痛影响问卷——修订后的总分FIQR [22]。总分结合了三个领域的分量表:功能、整体影响和症状。参与者每周完成 FIQR、疼痛VAS和多感官敏感性评分,持续 10 周,并在最后随访的4周内每周完成一次。本研究的次要数据结果多维疲劳评估 (MAF) 问卷[ 23 , 24 ] 是美国风湿病学会推荐的用于衡量风湿病状况下疲劳的量表 [ 25]。MAF 在基线、5周、10周和治疗后4周进行。所有评估均通过REDCap以电子方式进行。
统计分析
主要和次要结果分析:所有分析均在意向治疗的基础上进行。因为有3名中途退出研究的参与者,我们根据当前数据的曲线方法对缺失数据进行建模,将分数截断为前六个月报告的最高和最低疼痛评分(在基线时收集)。我们进行了随机效应GLS回归,基线疼痛和基线治疗预期作为固定效应和时间 x 组分配为随机效应。为了控制异方差性和面板内序列相关性,进行稳健分析。为每个模型计算了随机效应的 Breusch-Pagan-LaGrange乘数。所有次要分析都经Holm-Bonferroni校正,分析由对分组不知情的SM进行。使用Stata 软件13.1版(College Station,TX,USA)完成统计分析。
资金来源:该研究 (K23AT006392) 由美国国立卫生研究院国家补充和综合健康中心资助。该方案由作者制定,由临床研究事务办公室审查。
该研究得到了俄勒冈健康与科学大学机构审查委员会的批准,ClinicalTrials.gov 上注册(NCT02053090)。
结果
参与者的基线特征:共有30名参与者被随机分为两组,其中针灸组16人,教育组14人。第一个受试者于2014年9月招募,最后一次随访于2015 年7月进行。这些女性主要是非西班牙裔白种人 (87.1%),平均年龄为 54 岁。基线 FIQR 总分 (SD) 为 51.4 (15.5),表明负面影响程度很高。全球疲劳指数为 36.1(6.7)。教育组和针灸组的基线疼痛(问题 12)得分分别为 6.2(1.8)和 6.3(1.4)。两组患者在年龄、针灸预期、BMI 和基线 FIQR 总分方面没有显着差异。所有参与者的中医辨证为气血瘀滞、气血两虚或肝气郁结。这是由两名针灸师(SM 和 CW)在筛选访问时确定的。鉴于此标准,没有排除其他参与者(表格1)

干预、出勤和依从性
针灸组完成了83.3%的治疗和98.1%的评估。教育组的治疗完成率和评估完成率相似,分别为96%和91%。这表明参与者对两种治疗方案都比较认可。
两组均未发生与治疗方案或研究参与相关的意外不良事件。针灸组中的1人报告有瘀伤(<1%的治疗),并且有1例头晕在静坐三分钟后得到缓解。CONSORT 图显示了参与者流程(图1)。

三名参与者中途退出,两名在教育组(新工作和与本研究无关的手术),一名在针灸组(辍学)。对他们的数据进行建模。
主要结果分析——FIQR 总计
基线数据中,两组患者疼痛、BMI、年龄和针灸预期没有差异。 教育组患者在治疗结束和 4 周的随访中没有改善 ( P = 0.50)。针灸组患者在经过群体针灸治疗后显著改善(P < 0.001) FIQR 总分,在治疗结束时(10 周)的建模平均改善为17.3,在4周的随访中继续改善,平均改善为22.3。这些分别代表整体纤维肌痛影响的34%和43%的改善。所有模型的随机效应的 Breusch-Pagan-LaGrange 乘数均显着(P < 0.001),表明随机效应模型是正确的(表 2A)

次要结果测量
两组患者的全球疲劳指数 (GFI)在基线无差异。教育组患者GFI上的改善不显着。针灸组患者GFI 则显着改善 ( P < 0.001)。他们报告在治疗结束时改善了25%,在治疗后4周改善了33%(表 2B和图 2)。 图 2显示带有拟合线和标准偏差的原始数据。


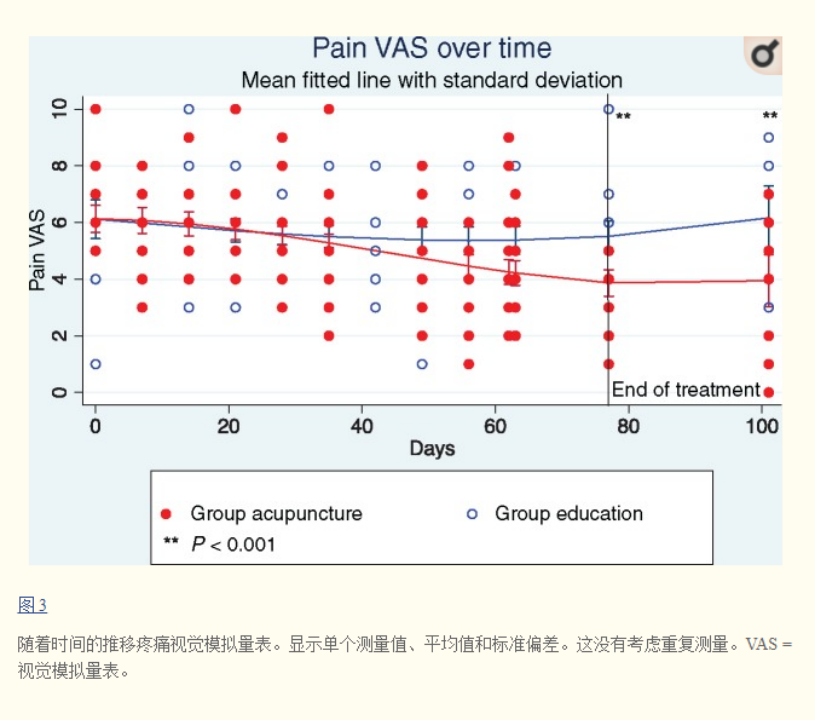
疼痛VAS:针灸组患者治疗后与基线相比,疼痛平均减少了2.8次,在为期4周的随访中进一步降至3.5次。(图3)。
讨论
本研究设计有两个特点,干预措施是在小组环境下提供给患者的,另外就是中医辨证取穴。群体针灸是一种在亚洲经常使用的治疗模式。该模式对于纤维肌痛患者来说是一种有效的治疗方式。原因分析如下:首先,运用中医辨证取穴进行患者个体化。虽然纤维肌痛是一个简单的诊断,但患有纤维肌痛的患者个体可以有几种不同的不适表现 [15],根据患者的不同症状选取不同的针灸穴位采取不同的治疗方法。第二个原因可能是治疗过程中的群体化。众所周知,纤维肌痛人群缺乏社交网络,在群体治疗中,患者通常会与其他参与者建立关系 [28]。在群体教育中,通常是由一位经验丰富的纤维肌痛研究人员为主导进行小组讨论,但内容上没有深远的改进。这意味着,如果治疗的群体性质很重要,但群体教育却达不到有效的治疗效果,治疗效果还是和治疗方案相关。
本研究还有两个缺陷:随访时间和针灸师人数有限。这项研究的随访时间仅为干预后 4 周。在最近的针灸研究学会会议上,几位学者建议所有针灸研究都应有至少六个月的随访期,最好是一到两年 [ 35 , 36 ]。据观察,在大多数疼痛研究中,对针灸有反应的人的治疗效果持续改善长达一年 [36]。
群体针灸有效的改善了纤维肌痛患者的疼痛和疲劳,因此我们建议,在治疗纤维肌痛时应该考虑在群体环境中进行个体化针灸。本研究中患者有相对较高的疼痛评分,而单凭药物方法无法解决这一问题。许多参与者说他们的生活有所改善,和10周前对比,疲劳和疼痛减少了近一半。虽然需要研究更大和更多样化的人群,但对于那些无法控制症状的人来说,群体针灸应该被视为一种治疗选择。
总之,我们的研究提供了初步证据,表明基于群体中医辨证的针灸可以改善纤维肌痛、疼痛和疲劳的负面影响。鉴于针灸的安全性和相对较少的副作用,它应该被视为治疗纤维肌痛患者的一种治疗选择。
编译、审校:张陈麟
参考文献:
1. Wolfe F, Smythe HA, Yunus MB, et al. The American College of Rheumatology 1990 criteria for the classification of fibromyalgia. Report of the multicenter criteria committee. Arthritis Rheum 1990;332:160–72. [PubMed] [Google Scholar]
2. Wolfe F, Clauw DJ, Fitzcharles MA, et al. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthrit Care Res 2010;625:600–10.http://dx.doi.org/10.1002/acr.20140 [PubMed] [Google Scholar]
3. Walitt B, Nahin RL, Katz RS, et al. The prevalence and charcteristics of fibromyalgia in the 2012 National Health Interview Survey. PLoS One 2015;109:e0138024. [PMC free article] [PubMed] [Google Scholar]
4. Arnold LM, Clauw DJ, McCarberg BH.. Improving the recognition and diagnosis of fibromyalgia. Mayo Clin Proc 2011;865:457–64.http://dx.doi.org/10.4065/mcp.2010.0738 [PMC free article] [PubMed] [Google Scholar]
5. Annemans L, Le Lay K, Taieb C.. Societal and patient burden of fibromyalgia syndrome. Pharmaeconomics 2009;277:547–59.http://dx.doi.org/10.2165/11313650-000000000-00000 [PubMed] [Google Scholar]
6. Berger A, Dukes E, Martin S, Edelsberg J, Oster G.. Characteristics and healthcare costs of patients with fibromyalgia syndrome. Int J Clin Practice 2007;619:1497–508. [PMC free article] [PubMed] [Google Scholar]
7. Konvicka JJ, Meyer TA, McDavid AJ, Robertson CR.. Complementary/alternative medicine use among chronic pain clinic patients. J Perianesth Nurs 2008;231:17–23. [PubMed] [Google Scholar]
8. de Miguel C, Campayo AJ, Flórez MT, et al. Interdisciplinary consensus document for the treatment of fibromyalgia. Actas Esp Psiquiatr 2010;2:108–20. [PubMed] [Google Scholar]
9. Lauche R, Cramer H, Hauser W, Dobos G, Langhorst J.. A systematic overview of reviews for complementary and alternative therapies in the treatment of fibromyalgia syndrome. Evid Based Complment Alternat Med 2015;2015:610–5. [PMC free article] [PubMed] [Google Scholar]
10. Martin-Sanchez E, Torralba E, Diaz-Dominguez E, Barriga A, Martin JL.. Efficacy of acupuncture for the treatment of fibormyalgia: Systematic review and meta-analysis of randomized trials. Open Rheum J 2009;31:25–9. [PMC free article] [PubMed] [Google Scholar]
11. Mayhew E, Ernst E.. Acupuncture for fibromyaliga—a systematic review of randomized clinical trials. Rheumatology 2007;465:801–4. [PubMed] [Google Scholar]
12. Deare J, Zheng CZ, Xue CC.. Acupuncture for treating fibromyaliga. Cochrane Database Syst Rev 2013;(5):CD007070. [PMC free article] [PubMed] [Google Scholar]
13. Langhorst J, Klose P, Musial F, Irnich D, Häuser W.. Efficacy of acupuncture in fibromyaliga syndrome: A systematic review with a meta-analysis of controlled clinical trials. Rheumatology 2010;494:778–88. [PubMed] [Google Scholar]
14. Mist SD. Prediction of Traditional Chinese Medicine Diagnosis from Psychosocial Questionnaires. Saarbrucken: LAP Lambert Academic Publishing; 2011. [Google Scholar]
15. Mist SD, Wright C, Jones KD, Carson JW.. Traditional Chinese Medicine diagnosis in a sample of women with fibromyalgia. Acupunt Med 2011;294:266–9.http://dx.doi.org/10.1136/acupmed-2011-010052 [PMC free article] [PubMed] [Google Scholar]
16. Ritenbaugh D, Hammerschlag R, Dworkin SF, et al. Comparative effectiveness of traditional Chinese medicine and psychosocial care in the treatment of temporomandibular disorders-associated chronic facial pain. J Pain 2012;1311:1075–89.http://dx.doi.org/10.1016/j.jpain.2012.08.002 [PMC free article] [PubMed] [Google Scholar]
17. Beck AT, Ward C, Mendelson H, Mock MJ, Erbaugh J.. An inventory for measuring depression. Arch Gen Psychiatry 1961;4:561–71.http://dx.doi.org/10.1001/archpsyc.1961.01710120031004 [PubMed] [Google Scholar]
18. Aickin M. A simulation study of the validity and efficiency of design-adaptive allocation to two groups in the regression situation. Int J Biostat 2009;51:19. [PMC free article] [PubMed] [Google Scholar]
19. Aickin M. Randomization, balance, and the validity and efficiency of design-adaptive allocation methods. J Stat Plann Inference 2001;941:92–119. [Google Scholar]
20. Aickin M. A program for balancing the allocation of subjects to treatment in a clinical trial. Comp Biomed Res 1982;156:519–24.http://dx.doi.org/10.1016/0010-4809(82)90014-3 [PubMed] [Google Scholar]
21. Mist SD, Ritenbaugh C, Aickin M.. Effects of questionnaire-based diagnosis and training on inter-rater reliability among practitioners of Traditional Chinese Medicine. J Altern Complment Med 2009;157:703–9.http://dx.doi.org/10.1089/acm.2008.0488 [PMC free article] [PubMed] [Google Scholar]
22. Liptan G. Figuring out Fibromyalgia: Current Science and the Most Effective Treatments, 1st edition.Portland, OR: Visceral Books; 2011. [Google Scholar]
23. Bennett RM, Friend R, Jones KD, et al. The Revised Fibromyaliga Impact Questionnaire (FIQR): Validation and psychometric properties. Arthritis Res Ther 2009;114:R120. [PMC free article] [PubMed] [Google Scholar]
24. Hewlett S, Hehir M, Kirwan JR.. Measuring fatigue in rheumatoid arthritis: A systematic review of scales in use. Arthritis Rheum 2007;573:429–39.http://dx.doi.org/10.1002/art.22611 [PubMed] [Google Scholar]
25. Belza B, Henke C, Yelin E, Epstein W, Gilliss C.. Corralates of fatigue in older adults with rheumatoid arthritis. Nurs Res 1993;422:93–9. [PubMed] [Google Scholar]
26. American College of Rheumatology. Multidimentional Assessment of Fatigue—MAF. Available at: http://www.rheumatology.org/I-Am-A/Rheumatologist/Research/Clinician-Researchers/Multidimensional-Assessment-of-Fatigue-MAF (Accessed August, 2017).
27. Feiveson A. How can I use Stata to calculate power by simulation? StataCorp LLC. Available at: https://www.stata.com/support/faqs/statistics/power-by-simulation/ (accessed August 2017).
28. Holm S. A simple sequentially rejective multiple test procedure. Scand J Stat 1979;62:65–70. [Google Scholar]
29. Aickin M, Gensler H.. Adjusting for multiple testing when reporting research results: The Bonferroni vs Holm Method. Am J Public Health 1996;865:726–8.http://dx.doi.org/10.2105/AJPH.86.5.726 [PMC free article] [PubMed] [Google Scholar]
30. Jones KD, Liptan GL.. Exercise interventions in fibromyalgia: Clinical applications from the evidence. Rheum Dis Clin N Am 2009;352:373–91.http://dx.doi.org/10.1016/j.rdc.2009.05.004 [PubMed] [Google Scholar]
31. Ioannidis J. Why most discovered true associations are inflated. Epidemiology 2008;195:640–8.http://dx.doi.org/10.1097/EDE.0b013e31818131e7 [PubMed] [Google Scholar]
32. Harris RE, Tian X, Williams DA, et al. Treatment of fibromyalgia with formula acupuncture: Investigation of needle placement, needle stimulation, and treatment frequency. J Altern Complement Med 2005;114:663–71.http://dx.doi.org/10.1089/acm.2005.11.663 [PubMed] [Google Scholar]
33. Assefi NP, Sherman K, Jacobsen J, et al. A randomized clinical trial of acupuncture compared with sham acupuncture in fibromyalgia. J Rehab Med 2008;407:582–8. [Google Scholar]
34. Cao JQ, Li Y.. Combination of acupunctuer and antidepressant medications in treatment of 56 cases of fibromyaliga. Chin Arch Trad Chin Med 2003;215:813–7. [Google Scholar]
35. Cao H, Li X, Han M, Liu J.. Acupoint stimulation for fibromyalgia: A systematic review of randomized controlled trials. Evid Based Complement Alternat Med 2013;2013:362831.. [PMC free article] [PubMed] [Google Scholar]
36. Sprott H. Efficiency of acupuncture in patients with fibromyalgia. Clin Bull Myofac Ther 1998;31:37–43.http://dx.doi.org/10.1300/J425v03n01_05 [Google Scholar]
37. MacPherson H. Specific effects for acupuncture—where do we stand, where should we go? J Complement Alternat Med 2016;221:A1–46. [Google Scholar]
38. Witt C. Innovative clinical acupuncture resaerch: From RCT’s to comparative effectiveness research. J Alternat Complement Med 2016;221:A1–46. [Google Scholar]
39. Mist SD, Jones K.D, Bennett RM.. Psychometrics of Online Adminstration of the Revised Fibromyalgia Impact Questionnaire. San Francisco: American College of Rheumatology; 2015. [Google Scholar]
40. Martenson ME, Halawa OI, Tonsfeldt KJ, et al. A possible neural mechanism for photosensitivity in chronic pain. Pain 2016;1574:868–78.http://dx.doi.org/10.1097/j.pain.0000000000000450 [PMC free article] [PubMed] [Google Scholar]
41. Deluze C, Bosia L, Zirbs A, Chantraine A, Vischer TL.. Electroacupuncture in fibromyalgia: Results of a controlled trial Brit Med J 1992;3056864:1249–52. [PMC free article] [PubMed] [Google Scholar]
声明:古麻今醉公众号为舒医汇旗下,古麻今醉公众号所发表内容之知识产权为舒医汇及主办方、原作者等相关权利人所有。未经许可,禁止进行转载、摘编、复制、裁切、录制等。经许可授权使用,亦须注明来源。欢迎转发、分享。
不感兴趣
看过了
取消

 打赏
打赏
不感兴趣
看过了
取消
精彩评论
相关阅读




中国医院排行榜















 010-82736610
010-82736610
 股票代码: 872612
股票代码: 872612



©2012-2023 北京华媒康讯信息技术股份有限公司 All Rights Reserved. 注册地址:北京 联系电话:82736610
 京公网安备 11010802020745号
京公网安备 11010802020745号


