
预计根据KTA框架创建和转化知识的各种拟议活动可被(新)护士用于促进临床环境中EBP的吸收、使用和实施,从而缩小知识与实践之间的差距。
Full text
Globally, nurses are expected to base their practices on rigorous evidence to improve individual patients’ health outcomes and the overall quality of health care. Therefore, the use, uptake and implementation of best practices, such as evidence-based health practices, methods, interventions, procedures or techniques are increasingly encouraged in an attempt to provide the best care possible in an environment that has become progressively more complex (Lehane et al 2019). Evidence-based practice (EBP) requires nurses to incorporate the best research with clinical proficiency and patient values to achieve optimal health outcomes (Lehane et al. 2019; Winters & Echeverri 2012). However, it takes on average 17 years for best practices to be implemented in clinical practice (Green et al. 2009), which can be referred to as the so-called ‘knowledge-practice gap’. Although nursing students are introduced to the concept of EBP at an early stage during their nursing education, and there is an expectation for nurses to use, uptake and implement best practices, this often does not happen because of various reported barriers, including lack of time, staff shortages, heavy patient caseloads, limited knowledge of EBP and negative beliefs towards EBP as well as limited academic skills, which seems especially to be the case for novice nurses (Ferguson & Day 2007; Mallion & Brooke 2016).
Knowledge translation is used to close the knowledge-practice gap and can be defined as translating clinical science, knowledge or evidence, which aims to enhance health outcomes (Grimshaw et al. 2012; Steinskog et al. 2021). The Knowledge-to-Action (KTA) Framework was developed based on consensus of 31 planned-action theories (the action cycle) as well as the knowledge creation component to offer a holistic view of knowledge translation (Graham & Tetroe 2010). The KTA framework consists of two main components: Knowledge Creation and the Action Cycle. The Knowledge Creation process is divided into three phases: (1) knowledge inquiry, (2) knowledge synthesis and (3) knowledge tools and products, whereas the Action Cycle focuses on application of knowledge in the practice setting, using seven phases, namely: (1) identifying problem or gap that needs attention and identify, review and select the knowledge (evidence) that can solve that problem or gap; (2) adapting or tailoring the knowledge obtained to the local context; (3) assessing barriers and facilitators to knowledge use; (4) selecting, tailoring and implementing the tailored interventions; (5) monitoring the knowledge use after implementation of the interventions; (6) evaluating outcomes on the interventions’ target group and (7) sustaining the knowledge use (Graham & Tetroe 2010) (see Figure 1).
FIGURE 1
The Knowledge-to-Action framework.
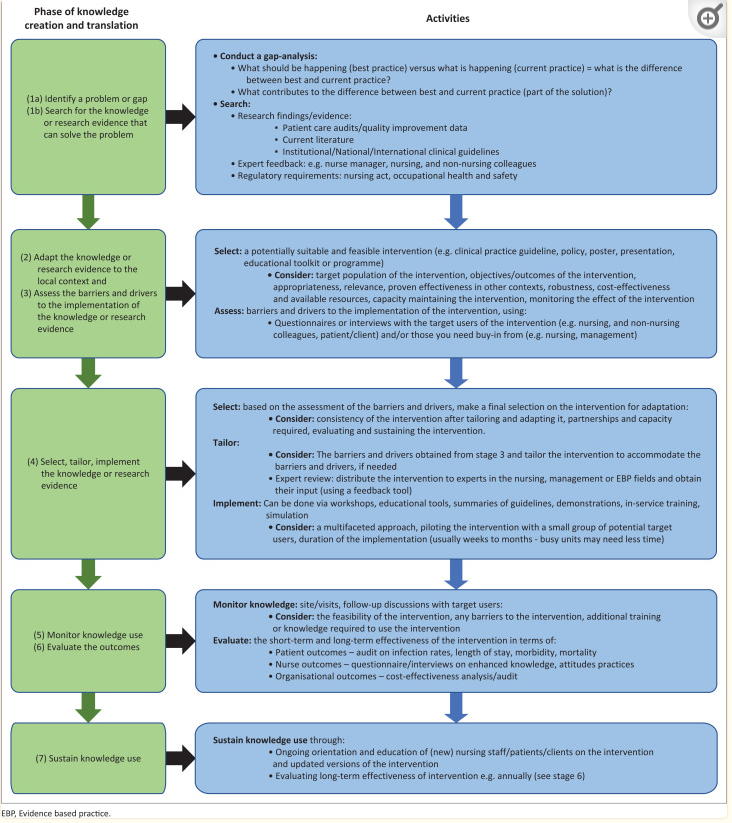
Figure 2 illustrates how the KTA framework can be used by (novice) nurses for the uptake, use and implementation of EBPs in clinical practice.
FIGURE 2
Utilisation of the knowledge-translation-action framework.
Some side notes need to be made to the proposed activities in relation to the KTA framework in Figure 2. The proposed activities are not fully comprehensive and may be adapted, depending on the knowledge translation context. Further, the distinction between adaptation of the knowledge (stage 2) and selecting the knowledge (stage 4) is not always clear or may seem repetitive; however, considering adaptability from the earliest stages of knowledge translation could help ensure that interventions are more resilient to changes in the context. Additionally, stakeholder involvement to create a sense of ownership, leadership, a feasible and contextually appropriate plan or strategy on how to implement the intervention, as well as buy-in as overarching principles should be central to all stages of knowledge translation (Moore et al. 2021). It is further recommended that novice nurses should be mentored and trained by, for example, senior nurses or academics on EBP, and active partnership and collaboration between (novice) nurses and academics must be promoted, especially as limited knowledge of EBP and limited academic skills were reported barriers towards the uptake, use and implementation of EBPs (Mallion & Brooke 2016). Nonetheless, it is expected that the various proposed activities to create and translate knowledge according to the KTA framework could be used by (novice) nurses to promote the uptake, use and implementation of EBPs in clinical settings, thereby reducing the knowledge-practice gap.
全文翻译(仅供参考)
从全球范围来看,护士的实践都被期望建立在严格证据的基础上,以改善个体患者的健康结局和整体医疗质量,因此,最佳实践的使用、吸收和实施,如循证健康实践、方法、干预、越来越多地鼓励在已经变得越来越复杂的环境中尝试提供可能的最佳护理的程序或技术(Lehane等人2019循证实践(EBP)要求护士将最佳研究与临床熟练程度和患者价值观相结合,以实现最佳健康结果(Lehane等人,2008年)。2019;温特斯&埃切韦里2012)。然而,在临床实践中实施最佳实践平均需要17年(绿色等人2009),这就是所谓的“知行差距”。虽然护生在接受护理教育的早期阶段已被引入EBP的概念,并期望护士使用、吸收和实施最佳实践,但由于种种障碍,包括时间不足、人手短缺、病人工作量大、EBP知识有限,对EBP持负面看法,以及学术技能有限,这似乎尤其是新手护士的情况(Ferguson & Day2007;马利安&布鲁克2016).
知识转化用于缩小知识与实践之间的差距,可定义为转化临床科学、知识或证据,旨在改善健康结果(Grimshaw等人,2012; Steinskog等人2021)。知识转化为行动(KTA)框架是基于31个计划行动理论(行动周期)的共识以及知识创造组件开发的,以提供知识转化的整体观点(Graham & Tetroe2010信托机构框架由两个主要部分组成:知识创造 和行动周期。知识创造 过程分为三个阶段:(1)知识查询,(2)知识综合,(3)知识工具和产品,而行动周期 侧重于知识在实践环境中的应用,分为七个阶段,即:(1)识别需要注意的问题或差距,并识别、审查和选择能够解决该问题或差距的知识(证据);(2)根据当地情况调整或修改所获得的知识;(3)评估知识使用的障碍和促进因素;(4)选择、调整和实施调整后的干预措施;(5)监测干预措施实施后的知识使用情况;(6)评估干预目标群体的结果;(7)持续使用知识(Graham & Tetroe2010).
需要对以下文件中与信托机构框架有关的拟议活动作一些补充说明。建议的活动并不完全全面,可能会根据知识翻译的背景进行调整。此外,调整知识(第2阶段)和选择知识(第4阶段)之间的区别并不总是明确的,或者可能看起来重复;然而,从知识转化的最早阶段就考虑适应性有助于确保干预措施更能适应环境的变化。此外,利益相关者的参与有助于建立一种主人翁意识、领导意识、一种可行的、适合环境的关于如何实施干预措施的计划或战略,以及作为支配性原则的认同应该是知识转化所有阶段的核心(Moore等人,2021)。此外,我们建议新护士应接受资深护士或学术界人士的指导及训练,并促进新护士与学术界人士之间的积极合作,特别是由于新护士对循证护理的知识有限及学术技能有限,是学习、使用及推行循证护理的障碍(Mallion及Brooke2016)。尽管如此,预计根据KTA框架创建和转化知识的各种拟议活动可被(新)护士用于促进临床环境中EBP的吸收、使用和实施,从而缩小知识与实践之间的差距。
THE
END
不感兴趣
看过了
取消

人点赞

人收藏

打赏
不感兴趣
看过了
取消
©2012-2023 北京华媒康讯信息技术股份有限公司 All Rights Reserved. 注册地址:北京 联系电话:010-82736610
广播电视节目制作经营许可证 —(京)字第 17437号 京海食药监械经营备20200522号
京ICP备12011723号 京ICP证150092号
 京公网安备 11010802020745号
工商备案公示信息
(京)网药械信息备字(2025)第00082号
京公网安备 11010802020745号
工商备案公示信息
(京)网药械信息备字(2025)第00082号

打赏金额
认可我就打赏我~
1元 5元 10元 20元 50元 其它
打赏作者
认可我就打赏我~
扫描二维码
立即打赏给Ta吧!
温馨提示:仅支持微信支付!
已收到您的咨询诉求 我们会尽快联系您































 010-82736610
010-82736610
 股票代码: 872612
股票代码: 872612




