
为了调整最佳剂量,在麻醉期间以体重为基础的剂量给予瑞马唑仑时模拟Ce是有利的。另老年患者可在低的瑞马唑仑Ce下恢复。
本文由“罂粟花"授权转载
全身麻醉期间反应丧失和恢复时瑞马唑仑的效应室浓度:一项模拟研究

贵州医科大学 麻醉与心脏电生理课题组
翻译: 安丽 编辑:潘志军 审校:曹莹
背景:瑞马唑仑是新型的一种超短效苯二氮卓类药物,与目前使用的催眠药相比,它具有起效快、作用时间短,可逆转和维持血流动力学稳定等优点,被越来越多地被用作全凭静脉麻醉(TIVA)。由于这些药理学特性,准确掌握瑞马唑仑浓度在麻醉实施中运用是有益的。本研究的目的是通过模拟全麻患者反应丧失(LOR)和反应恢复(ROR)时瑞马唑仑的效应室浓度(Ce),研究患者因素与LOR和ROR模拟时Ce之间的关系。
方法:回顾性分析了2021年8月4日至2021年10月12日期间81例在全身麻醉下使用瑞马唑仑(remimazolam)进行择期手术的患者的医疗记录。瑞马唑仑以6或12mg/kg/h为诱导剂量给予患者,直到患者反应消失,随后以0.3-2mg/kg/h维持,以保持BIS值在60以下。使用Asan泵软件模拟手动输注模式,并使用Schüttler模型模拟瑞马唑仑的Ce。无论何时手动改瑞马唑仑的输注速率,几乎同时可确认模拟Ce。在Asan程序中分别记录了“LOR”和“ROR”时的Ce。
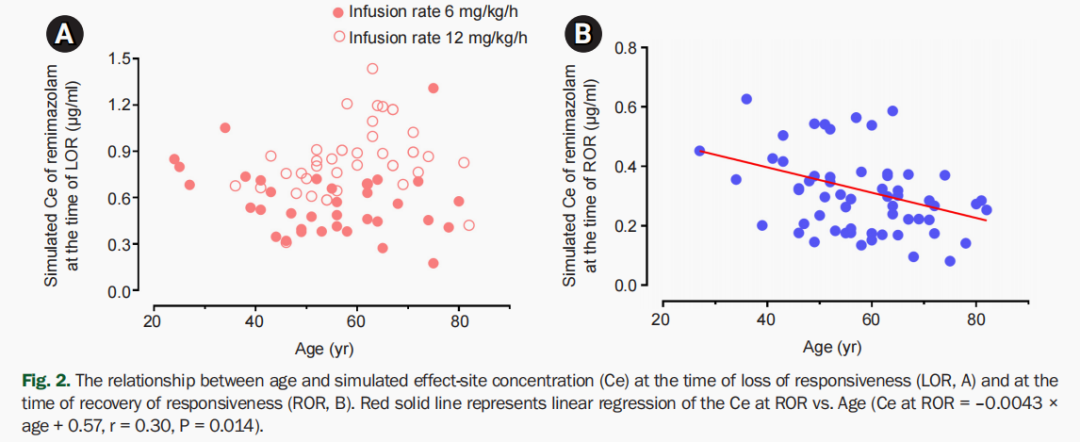
结果:在LOR和ROR时模拟Ce的中位数值(1Q、3Q)分别为0.7(0.5、0.9)和0.3(0.2、0.4)μg/ml。累积注射瑞马唑仑0.3 mg/kg,1.9分钟后达到LOR。年龄与ROR模拟Ce之间存在显著相关性(ROR时模拟Ce=-0.0043×年龄+0.57,r=0.30,P=0.014)。
结论:为了调整最佳剂量,在麻醉期间以体重为基础的剂量给予瑞马唑仑时模拟Ce是有利的。另老年患者可在低的瑞马唑仑Ce下恢复。
原始文献来源:
Kyung Mi Kim, Ji-Yeon Bang, Jong Min Lee, Hong Seuk Yang, Byung-Moon Choi, and Gyu-Jeong Noh.Effect-site concentration of remimazolam at loss and recovery of responsiveness during general anesthesia: a simulation study.Anesth Pain Med 2022;17:262-270.Doi.org/10.17085/apm.21121
英文原文:
Effect-site concentration of remimazolam at loss and recovery of responsiveness during general anesthesia:a simulation study
Abstract
Background: The objective of this study was to investigate the effect-site concentration (Ce) of remimazolam at loss of response (LOR) and recovery of response (ROR) in patients underwent general anesthesia using simulation. In addition, the relationships between patient’s factors and simulated Ce at LOR and ROR were examined.
Methods: The medical records of 81 patients who underwent elective surgery under general anesthesia using remimazolam with simulation of Ce between August 4, 2021 and October 12, 2021, were retrospectively reviewed. Remimazolam was administered as an induction dose of 6 or 12 mg/kg/h until the patient became unresponsive, followed by 0.3–2 mg/kg/h to maintain BIS values below 60. Simultaneously, simulations of manual infusion mode were performed using Asan Pump software and the Ce of remimazolam was simulated using the Schüttler model. Whenever infusion rate of remimazolam was manually changed, the simulated Ce was confirmed almost simultaneously. LOR and ROR, defined as unresponsive and eye-opening to verbal commands, respectively, were recorded in the Asan Pump program.
Results: The median (1Q, 3Q) simulated Ce at LOR and ROR were 0.7 (0.5, 0.9) and 0.3 (0.2, 0.4) μg/ml, respectively. LOR was achieved in 1.9 min after remimazolam infusion with cumulative doses of 0.3 mg/kg. There was a significant relationship between age and simulated Ce at ROR (Ce at ROR = –0.0043 × age + 0.57, r = 0.30, P = 0.014).
Conclusions: For optimal dosage adjustment, simulating Ce while administering remimazolam with a weight-based dose during anesthesia is helpful. Elderly patients may recover from anesthesia at lower Ce of remimazolam.
不感兴趣
看过了
取消

人点赞

人收藏

打赏
不感兴趣
看过了
取消
©2012-2023 北京华媒康讯信息技术股份有限公司 All Rights Reserved. 注册地址:北京 联系电话:010-82736610
广播电视节目制作经营许可证 —(京)字第 17437号 京海食药监械经营备20200522号
京ICP备12011723号 京ICP证150092号
 京公网安备 11010802020745号
工商备案公示信息
互联网药品信息服务资格证书((京)-非经营性-2020-0015)
京公网安备 11010802020745号
工商备案公示信息
互联网药品信息服务资格证书((京)-非经营性-2020-0015)






您已认证成功,可享专属会员优惠,买1年送3个月!
开通会员,资料、课程、直播、报告等海量内容免费看!

打赏金额
认可我就打赏我~
1元 5元 10元 20元 50元 其它
打赏作者
认可我就打赏我~
扫描二维码
立即打赏给Ta吧!
温馨提示:仅支持微信支付!
已收到您的咨询诉求 我们会尽快联系您






































 010-82736610
010-82736610
 股票代码: 872612
股票代码: 872612




