
我们的研究发现几种新的可能对于胆囊癌预后有重要意义的基因变化。这些发现的验证可能作用于潜在的靶向治疗,以改善这些毁灭性肿瘤患者的预后。
本文转载自复旦大学附属中山医院分子病理中心洞见分子,作者:HISTO PATH,翻译者:王语林
今年3月份“第111届美国和加拿大病理学会(USCAP)年会”以线下、线上会议相结合形式在美国洛杉矶举办。
美国和加拿大病理学会(USCAP)是病理学界最具影响力的国际学术组织之一,是全球病理学领域知识传播的全球领导者,拥有超过1万名病理学家会员。USCAP年会是世界上规模最大、最具影响力的病理学专业学术会议,每年都有数千名来自医院、私人实验室、学术机构和政府机构的病理学和分子、毒理学、肿瘤学和免疫学等相关专业领域的专业人士出席会议。
今年的会议在多个领域更新了分子病理前沿进展,内容丰富,为业界所瞩目。我们分子病理中心也选取了其中的一些精彩摘要进行翻译,与同道们分享交流。
一、导管内乳头状粘液性肿瘤和相关浸润性导管腺癌的免疫应答进展
结果:导管内乳头状粘液性肿瘤(IPMN)表现出被激活的免疫微环境(TME,tumor immune microenvironment),包括免疫抑制细胞和调节细胞的浸润:Foxp3+,CD68+以及免疫检查点蛋白的表达:LAF3,PD-1,PD-L1,VISTA。虽然在IPMN和浸润性PDAC之间未发现CD45+浸润细胞的差异,免疫细胞亚群在癌前病变发展至浸润性癌的过程中有明显的调节作用。相比IPMN,在相关浸润性PDAC中发现以下细胞亚群密度明显增加:CD68+细胞, p<0.001; Foxp3+ 细胞, p=0.04; LAG3+ 细胞, p=0.017;PD-L1+ 细胞, p=0.03。而CD20+, CD4+, CD8+, PD-1+,VISTA+细胞密度无明显差异。
结论:IPMN的浸润模式表明,PDAC中的免疫抑制性的免疫微环境可能在浸润性PDAC出现之前就存在了。当肿瘤从IPMN进展为PDAC,免疫细胞亚群随之进化,并伴随免疫抑制细胞和调节性免疫检查点蛋白的增加。在癌前病变中存在的免疫抑制,以及在PDAC发展中TME的调节,提示在对肿瘤的预防和治疗方面可以通过免疫治疗进行多个时间点的干预。对于了解何时以及如何使用免疫治疗来改变肿瘤发展不同阶段的免疫微环境还需要更多的研究。
1.Progression of the Immune Response in Matched Intraductal Papillary Mucinous Neoplasms and Associated Invasive Ductal Adenocarcinomas
(Naziheh Assarzadegan, Braxton Alicia, Dwayne Thomas, et al.)
Results: IPMNs demonstrated an active TME with infiltration of immunosuppressive and regulatory cells: Foxp3+ and CD68+ and expression of immune checkpoint proteins: LAG3, PD-1, PD-L1 and VISTA. While no overall difference in CD45+ infiltrating cells was seen between IPMN and matched invasive PDAC on average, there was marked modulation of immune cell subsets with progression from precursor lesion to invasion. The density of the following cell subsets increased significantly in PDAC as compared to their matched IPMN: CD68+ cells, p<0.001; Foxp3+ cells, p=0.04; LAG3+ cells, p=0.017 and PD-L1+ cells, p=0.03. No significant differences were seen in density of CD20+, CD4+, CD8+, PD-1+ or VISTA+ cells.
Conclusions: The infiltration pattern of IPMNs suggests that groundwork for the immunosuppressive TME in PDAC may begin far prior to the presence of an invasive PDAC. Immune cell subsets evolved as tumors progressed from IPMNs to PDAC in matched patients, with increases seen in immunosuppressive cells and in regulatory immune checkpoint proteins. The presence of immunosuppression in precursor lesions, paired with modulation of the TME as PDAC develops, suggests multiple time points for potential intervention with immune-based therapies, both in a prophylactic and treatment paradigm. Additional studies are crucial to best understand when and how immune-based treatments can be used to alter the TME at different stages of tumor development.
二、高肿瘤突变负荷帮助鉴别伴有生存期延长和肿瘤免疫力提高的一种胰腺癌特殊亚型
结果:中位数和平均肿瘤突变负荷值(TMB)分别是3.36和5.64。整体检测到12例TMB-H病例(中位数:14.025,范围:10.21-129),包括5例MSI-H病例(100%),5例长期生存病例(20%)和2例传统的微卫星稳定的胰腺导管腺癌。相比TMB-L病例,TMB-H胰腺导管腺癌患者T细胞密度增加,CD3+、CD4+ 、FOXP3-T细胞(P=0.0398)和DC-LAMP+树突细胞(DC;P=0.0093)。5例TMB-H病例(41.66%)PD-L1+,显出出不同的PD1/PD-L1染色模式。ARID1A-和ERBB3+在TMB-H病例中同样具有较高发生频率。TMB-H患者的总生存率在5-71个月(中位数:27个月),TMB-L患者的总生存率在3-161个月(中位数:13个月),P<0.001。
结论:高肿瘤突变负荷将患者从特殊亚型的PDAC中筛选出来,比如LTS(MSS)和MSI-H患者。他们的微环境表现出强烈的抗肿瘤免疫应答,由数量增加的DC细胞介导,DC细胞可以启动和调节T细胞应答,以及CD3+CD4+FOXP3-T细胞,已知可以对肿瘤细胞直接产生细胞毒作用并可以加强DC细胞。TMB-H胰腺导管腺癌通常伴有其他改变,比如微卫星不稳定(MSI)、DNA损伤应答和修复以及ERBB3-改变。这些结果表明伴有TMB-H的PDAC患者可能是组合治疗包括免疫治疗的良好候选人。
2.High Tumor Mutational Burden Identifies Specific Subsets of Pancreatic Cancer Patients with Prolonged Survival and Improved Anti-tumor Immunity
(Eva Karamitopoulou-Diamantis, Andreas Andreou, Anna-Silvia Wenning, et al.)
Results: Median and mean TMB values were 3.36 and 5.64 respectively. Overall, 12 TMB-high cases (median:14.025, range:10.21-129) were detected. They comprised all five MSI-high cases (100%), five LTSs (20%) and two conventional MSS PDACs (1.66%). TMB-high PDACs exhibited high T cell density and significantly increased CD3+CD4+FOXP3-T cells (P=0.0398) and DC-LAMP+dendritic cells (DC; P=0.0093), compared with TMB-low cases. Five TMB-high cases (41.66%) were also PD- L1+ exhibiting various PD1/PD-L1 staining patterns. ARID1A- and ERBB3-alterations were more frequent in TMB-high tumors. The OS of TMB-high cases ranged between 5-71 months (median:27), whereas that of the TMB-low cases between 3-161 months (median:13), P<0.001.
Conclusions: High TMB mostly identifies patients from specific PDAC-subsets such as LTS (MSS) and MSI-high cases. Their microenvironment displays strong anti-tumor immune response, mediated by increased DC counts, which have the capacity to initiate and regulate T cell responses, as well as CD3+CD4+FOXP3-T cells, known to exhibit direct cytotoxicity against tumor cells as well as potentiate the DCs. TMB-high PDACs frequently harbor other actionable alterations, such as defective mismatch repair (MSI) and DNA Damage Response and Repair (ARID1A), as well as ERBB3-alterations. These results suggest that PDAC-patients with TMB-high tumors might be good candidates for combinatorial treatments including immunotherapy.
向下滑动查看


三、PTEN基因缺失和GLUT1表达预测了胰腺神经内分泌肿瘤转移
结果:46例(13%)患者有PTEN异常表达,43例(12%)患者有GLUT1异常表达,17例(5%)患者有2种蛋白的异常表达,PTEN缺失和GLUT1过表达与较大的肿瘤体积、高WHO分级、晚期T分期、ATRX/DAXX缺失、同时性和异时性转移有关(p<0.02)。无同时转移的271例患者中,PTEN阴性和/或GLUT1阳性患者的5年无复发生存率为40%,而PTEN阳性/GLUT1阴性患者的无复发生存率为89%(p<0.01)。根据多变量分析,PTEN和/或GLUT1的异常表达是无复发生存率的不良预后因素,与肿瘤大小、WHO分级、淋巴管和神经侵犯、N分期、ATRX/DAXX缺失无关(p<0.01)。此外,PTEN、GLUT1、和/或ATRX/DAXX的异常表达患者的5年无复发生存率为47%,无PTEN、GLUT1、和/或ATRX/DAXX的异常表达患者的5年无复发生存率为94%(p<0.01)。因此PTEN、GLUT1、和/或ATRX/DAXX的异常表达是无复发生存率的独立不良预后因素(p<0.01)。
结论:胰腺神经内分泌肿瘤中PTEN缺失和GLUT1表达是患者预后不良的生物标志物;因此PTEN和VHL的基因组改变可能在胰腺神经内分泌肿瘤的发病机制中发挥重要作用。
3.Loss of PTEN and Expression of GLUT1 Predict the Metastatic Progression of Pancreatic Neuroendocrine Tumors
(Azfar Neyaz, Jasmijn Westendorp, Abigail Wald, et al.)
Results: Aberrant expression of PTEN, GLUT1, or both proteins were seen in 46 (13%), 43 (12%), and 17 (5%) PanNETs. Both loss of PTEN and overexpression of GLUT1 correlated with large tumor size, high WHO grade, advanced T-stage, loss of ATRX/DAXX, and presence of synchronous and metachronous metastases (p<0.02). Among 271 patients without synchronous metastasis, the 5-year RFS rate for PTEN-negative and/or GLUT1-positive patients was 40% as compared to 89% for PTEN-positive/GLUT1-negative patients (p<0.01). By multivariate analysis, aberrant expression for PTEN and/or GLUT1 was a negative prognostic factor for RFS, and independent of tumor size, WHO grade, lymphovascular and perineural invasion, N-stage, and ATRX/DAXX loss (p<0.01). Moreover, aberrant expression of PTEN, GLUT1, and/or ATRX/DAXX was associated with 5-year RFS rate of 47% as compared to 94% for patients without aberrant expression for these proteins (p<0.01), and remained an independent, negative prognostic factor for RFS (p<0.01).
Conclusions: Loss of PTEN and expression of GLUT1 in PanNETs represent prognostic biomarkers of poor patient outcome; thus, genomic alterations in PTEN and VHL may play a significant role in PanNET pathogenesis.
四、临床晚期KRAS野生型胰腺导管腺癌(PDA)的基因组学研究
结果:721例(7.6%)PDAC为KRAS野生型(KRASwt)和8723例(92.4%)PDAC为KRAS突变型(KRASm)。年龄相似,KRASwt在男性中更常见。基因组改变(GA,genomic alterations)x相似。对于目前无法靶向的基因组改变,KRASwt组中ARID1A和RB1的基因组改变频率更高,而KRASm组中以TP53、CDKN2A/B、MTAP、SAMD频率更高。除了在1.6%KRASm胰腺导管腺癌中已发现的KRAS G12C突变,目前一些潜在靶向基因在KRASwt中突变频率较高,包括ERBB2(扩增或短变异GA),BRAF、PIK3CA、FGFR1/2、PTEN、ATM。虽然频率较低,KRASwtzu 胰腺导管腺癌具有更高频率的与免疫检查点抑制剂有效性(IPCI)有关的生物标志物,包括PBRM1基因组突变和TMB>10个突变/Mb,而KRASm组胰腺导管腺癌患者有较高频率的PD-L1免疫组化低表达。
结论:PDA的治疗仍是一个重要的挑战。我们的研究结果证实了以往的文献报道,在KRAS野生型PDA中更常见到多个靶向基因和高TMB。此外,将PDAC分类为KRAS突变型和KRAS野生型可能在临床上利于总结基因组轮廓和可用的靶向治疗。我们的研究强调了全面基因组分析的重要性,以期找到包括融合基因在内的分子靶点,实现精准肿瘤学。
4.Genomic Landscape of Clinically Advanced KRAS Wild-Type Pancreatic Ductal Adenocarcinoma (PDA)
(Serenella Serinelli, Daniel Zaccarini, Vamsi Parimi, et al.)
Results: 721 (7.6%) PDAs were KRAS wild-type (KRASwt) and 8,723 (92.4%) PDAs were KRAS mutated (KRASm), Table 1. Ages were similar, KRASwt were more often male gender. GA/tumor were similar. For currently not targetable GA, KRASwt featured greater frequencies of ARID1A and RB1 GA and KRASm featured greater frequencies in TP53, CDKN2A/B, MTAP, and SMAD4. With the exception of the KRAS G12C GA identified in 1.6% of the KRASm PDA, greater frequencies in currently potentially targetable genes were seen selectively among KRASwt including GA in ERBB2 (amplifications and short variant GA), BRAF, PIK3CA, FGFR1/2, PTEN, and ATM. Although frequencies were low, the KRASwt PDA featured greater frequencies of biomarkers associated with immune checkpoint inhibitor efficacy (IPCI) including PBRM1 GA and TMB > 10 mutations/Mb although KRASm PDA had a higher frequency of PD-L1 low but not high IHC expression.
Conclusions: Therapeutic management of PDA remains an important challenge. Our results confirm those reported in the literature, according to which many targetable genes and a high TMB are significantly more common among KRAS wild-type PDAs. Moreover, classification of PDAs into KRAS mutated vs KRAS wild-type categories may be clinically beneficial in summarizing the genomic profile and the available targeted therapies. Our findings highlight the importance of comprehensive genomic analysis to find molecular targets including gene fusions for precision oncology.
向下滑动查看

五、导管内乳头状粘液性肿瘤和相关浸润性导管腺癌的免疫应答进展
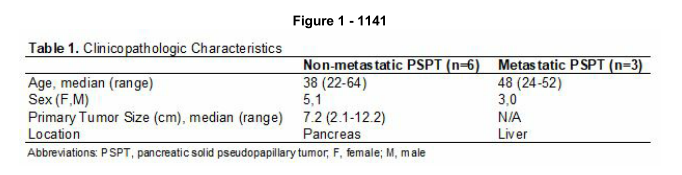
结果:9例PSPT患者的临床病理资料如表1所示。在所有PSPT病例中,RNA测序未发现明显的基因融合,但所有病例均表现出双等位基因CTNNB1第3外显子错义突变。所有病例的突变分析表明有101个基因突变为转移性PSPT特有,在非转移性PSPT患者中未发现。在101个基因中,下列3种基因可能作为肿瘤抑制基因参与肿瘤的转移过程:BLM、MYH9、PCK1。每个转移性PSPT病例表现出一种或多种上述基因的双等位基因突变,包括错义突变、移码突变、终止密码子提前、剪接供体、剪接受体或剪接区蛋白突变。MYH9的单一突变是根据一篇GeneReviews/OMIM数据库综述所确认的唯一致病突变。2种额外发现的突变基因,BLM、PCK1,在INVITA和Illumina数据库中其意义尚未确定。剩下的突变仍有未知的致病潜能。
结论:我们的研究表明,队列中所有非转移性/转移性PSPT患者都包含CTNNB1第3外显子的错义突变。此外,我们发现3种基因仅在转移性PSPT中突变,包括BLM、MYH9、PCK1,这些基因可能参与了肿瘤的转移进程。需要进一步调查以确定这3种基因是否在PSPT的转移性进展中发挥重要作用,是否与肿瘤的转移潜能有关。
5.BLM, MYH9, and PCK1 Mutations are Possible Markers of Metastatic Potential in Pancreatic Solid Pseudopapillary Tumors
(Benjamin VanTreeck, Hee Eun Lee, Colton McNinch, Lizhi Zhang)
Results: Clinicopathologic data for the 9 PSPT cases is summarized in Table 1. RNA sequencing revealed no significant gene fusions identified in all PSPT cases. All cases of PSPT demonstrated biallelic CTNNB1 missense mutations in exon 3. Variant analysis of all cases showed 101 gene mutations exclusively shared by metastatic PSPT that were not identified in nonmetastatic PSPT. Of the 101 genes, the following 3 genes may potentially act as tumor suppressors and participate in metastatic progression: BLM, MYH9, and PCK1. Each case of metastatic PSPT demonstrated one or more biallelic mutations in each of the previously mentioned genes leading to missense, frameshift, stop gained, splice donor, splice acceptor, or splice region protein alterations.
A single mutation in MYH9 (c.5797C>T) is the only confirmed pathogenic mutation based on a review in GeneReviews/OMIM databases. Two addition mutations, BLM (c.377C>T) and PCK1 (c.228G>T), each have an uncertain significance in INVITAE and Illumina databases, respectively. The remaining mutations have an unknown pathogenic potential.
Conclusions: We demonstrated that all non-metastatic and metastatic PSPT in our cohort contain a CTNNB1 missense mutation in exon 3. Furthermore, we identified 3 genes only mutated in metastatic PSPT, BLM, MYH9, and PCK1, that may potentially participate in PSPT metastatic progression. Additional investigation is required to determine if these 3 genes play a significant role in PSPT metastatic progression and are definitively associated with metastatic potential.
六、胰腺导管腺癌、肝内外胆管癌的基因组分析
背景:在原发不明的恶性肿瘤的研究中,鉴别胰腺导管腺癌PDC和胆管癌CCA具有挑战性,因为两者形态上相似,并且缺少免疫组化标记。这一鉴别对于治疗和预后有重要影响。这些肿瘤的基因组分析已被描述。肝内和肝外胆管癌(iCCA,eCCA)具有不同的分子特征。iCCA中IDH1/2突变、BAP1突变和FGFR2融合多见,而eCCA和PDC中TP53和KRAS具有较高的突变率。在这项研究中,我们直接比较了iCCA,eCCA和PDC的分子特征,以用于这些肿瘤的鉴别诊断。
设计:61例病例(39PDC,12iCCA,10eCCA)使用自定义设计的213基因二代测序进行检测。为了检测基因融合,使用了市售的FusionPlex CTL panel (ArcherDx)。从显微切割、福尔马林固定和石蜡包埋组织中提取总核酸,用于NGS检测,并在Illumina NextSeq进行测序。数据分析使用BWA和Pisces V2 (Illumina)用于变式调用(variant calling),ArcherDx软件用于融合,以及内部自定义的拷贝数变异(CNV)。
结果:该队列研究的人口统计数据见表1。所有肿瘤中检测到的体细胞突变见图1。IDH1突变、BAP1突变和FGFR2融合在iCCA中更常见;eCCA和PDC具有相似的突变特征,70-80%病例中有TP53和KRAS突变。KRAS G12R(9)和Q61H(3)只在PDC病例中被检测到;G12C在2例eCCA,G13D在1例iCCA中被检测到,见图2。在4/11的iCCA中检测到基因重排,(3例为FGFR/BICC1,1例为FGFR/SORBS1),eCCA和PDC中未检测到融合。CNV分析显示CDKN2A/B在18%的PDC病例、1例eCCA中缺失,iCCA病例中无缺失。4例有BAP1突变的病例在IHC中表现为BAP1缺失,而4例IHC中表达BAP1的病例无BAP1突变。
结论:我们的数据显示病例中有IDH1突变、BAP1突变和FGFR2融合支持iCCA的诊断。具有CDKN2A/B缺失或SMAD4缺失、ATM突变的肿瘤更倾向诊断PDC。我们的结果也支持以往CCA和PDC相关的分子研究。在研究中观察到两种肿瘤在KRAS突变存在差异,这一发现值得进一步研究。
6.Genomic Profiling of Pancreatic Ductal Adenocarcinoma, Intrahepatic and Extrahepatic Cholangiocarcinoma
(Matthew Gosse, Ramakrishna Sompallae, Natalya Guseva, et al.)
Background: In the work up of a carcinoma of unknown primary, the distinction between pancreatic ductal adenocarcinoma (PDC) and cholangiocarcinoma (CCA) is a challenging endeavor due the overlap in morphology and lack of immunohistochemistry (IHC) markers. The distinction has important ramifications for treatment and prognosis. Genomic analyses of these tumor types have been described. Intra- and extra-hepatic cholangiocarcinoma (iCCA and eCCA) had distinct molecular profiles. iCCA are enriched in IDH1/2 and BAP1 mutations and FGFR2 fusions whereas eCCA and PDC had a higher rate of TP53 and KRAS mutations. In this study, we directly compared molecular profiles of our institutional cohort of iCCA, eCCA, and PDC to aid in the distinction of the
diagnosis of these neoplasms.
Design: Sixty-one cases (39 PDC, 12 iCCA, and 10 eCCA) were tested using a custom-designed 213-gene next generation sequencing panel. For detection of gene fusions, the commercially available FusionPlex CTL panel (ArcherDx) was used. Total nucleic acid extracted from microdissected, formalin-fixed, paraffin-embedded tissue was used to generate NGS libraries and sequencing was performed on Illumina NextSeq. Data were analyzed using the BWA and Pisces v2 (Illumina) for variant calling, ArcherDx software for fusion, and an in-house built custom pipeline for copy number variation (CNV).
Results: The demographics of the cohort are shown in Table 1. Somatic mutations detected in all tumors are summarized in Fig. 1. Mutations in IDH1 and BAP1, and FGFR2 fusions were most commonly detected in iCCA; eCCA and PDC shared a similar mutation profile of TP53 and KRAS variants present in 70-80% of cases. KRAS G12R (9) and Q61H (3) were only detected in PDC; G12C in 2 eCCA, and G13D in 1 iCCA (Fig. 2). Gene rearrangements were detected in 4/11 iCCAs (3 with FGFR/BICC1 and 1 with FGFR/ SORBS1). No fusions were detected in eCCA (10) or PDC (32). CNV analysis showed CDKN2A/B loss in 18% PDC (n=39), 1 eCCA (n=12) and none in iCCA (n=10). All 4 iCCAs with BAP1 mutations showed BAP1 lost by IHC and all 4 cases of intact BAP1 expression by IHC showed no BAP1 mutation.
Conclusions: Our data show that the presence of IDH1, BAP1 mutation and FGFR2 fusion supports the diagnosis of iCCA. Tumors with loss of CDKN2A/B and/or SMAD4 and ATM mutations were most likely PDC. Our results support the previous molecular findings in CCA and PDC. The difference in KRAS variants in these two tumor types observed in this small cohort also warrants further investigation.



七、胆囊癌靶向基因组分析
背景:胆囊癌GBC经常在疾病晚期发现,预后不良。选择靶向治疗的突变是有限的。利用GBC突变基因进行二代测序可能会为临床治疗提供参考。目前的研究指出了GBC病例中二代测序检测的肿瘤相关基因与其临床病例特征的联系。
设计:对37例GBC患者的石蜡包埋FFPE组织中提取DNA,进行高深度、均匀覆盖的测序,(ION, Personal Genome),使用一个与大肠癌相关的22基因panel进行分析。胚系突变使用变体识别从血液和非肿瘤对照样本中进行筛选。
结果:共检测到178个突变,平均每个肿瘤有4.8个突变(范围1-15)。在SMAD4 (60.60%), NOTCH1 (45.45%), ERBB2 (45.45%), PIK3CA (33.33%) and MET (30.30%), PTEN (30.30%), EGFR (24.24%), KRAS (21.21%), BRAF (9.09%) and NRAS (6.06%) 检测到38个具有个性化治疗潜能的体突变。在66.7%(2/3)突变相关病例中淋巴结转移不明显。在2/3患者中BRAF基因突变与PIK3CA、TP53和EGFR基因突变互斥。在GBC中还观察到EGFR、KRAS和NRAS的热点突变,在结肠癌中也存在(见表1)。表1进一步详细说明了共存的突变。EGFR阳性的病例中有3/8例发生KRAS突变。TP53突变与组织病理分化相关(P=0.0001),ERBB4&ALK突变与坏死相关(P=0.012,0.027),EGFR突变和粘液性肿瘤相关(P=0.023),ERBB2基因突变和T分期相关(P=0.036)。脉管侵犯、神经浸润和淋巴结转移没有显著的遗传相关性。
结论:该研究为胆囊肿瘤的遗传改变和参与通路提供了一个概述。89.1%病例存在靶向突变,包括SMAD4, NOTCH1, ERBB2&4, PIK3CA, MET, PTEN, EGFR, KRAS, BRAF ,NRAS,与结肠癌基因突变存在重叠。这一研究支持了跟随结肠癌治疗运用基因图谱靶向治疗胆囊癌的可能性。
7.Targeted Genomic Profiling of Gallbladder Carcinoma
(Nuzhat Husain, Sridhar Mishra, Swati Kumari, et al.)
Background: Gallbladder cancer (GBC) often presents in late stage of disease with poor prognosis. Mutations for selection of targeted therapies are limited. Next-generation sequencing (NGS) using frequently mutated genes for GBC may provide a reference for clinical management. The current study identifies cancer-related genetic alterations by NGS in cases of GBC and their association with clinicopathological features.
Design: DNA from FFPE tissue of 37 cases of GBC was sequenced to high depth, uniform coverage (ION, Personal Genome Machine) and analysed for genomic alterations using a 22 gene panel related to colorectal cancer. The germline variants were filtered using variant calls from blood and non-tumor control samples.
Results: A total of 178 alterations were identified for an average of 4.8 alterations per tumor (range 1–15). A total of 38 different genomic alterations with the potential to personalize therapy in SMAD4 (60.60%), NOTCH1 (45.45%), ERBB2 (45.45%), PIK3CA (33.33%) and MET (30.30%), PTEN (30.30%), EGFR (24.24%), KRAS (21.21%), BRAF (9.09%) and NRAS (6.06%) gene. In 66.67% (2/3) co-mutated cases lymph node metastasis was not evident. BRAF gene mutation was mutually exclusive with PIK3CA, TP53 (n=3/3) and EGFR in 2/3 patients. Hot spot mutations of EGFR, KRAS and NRAS as seen in colorectal cancers were also observed in GBC (Table 1).Table 1 further details coexisting mutations. KRAS mutation was observed in 3/8 in EGFR positive cases. TP53 mutation was associated with histopathological differentiation (p=0.0001), ERBB4 & ALK mutation was associated with necrosis (p=0.012, 0.027), EGFR mutation was associated with mucinous tumors (p=0.023) and ERBB2 gene mutation was associated with T stage (p=0.036). No significant correlation of genetic profile with lympho-vascular invasion, perineural invasion, lymph-node metastasis was observed.
Conclusions: The current study provides an overview of genetic alterations and pathways involved in gallbladder tumorigenesis. Targetable mutations were identified in 89.91% cases and included SMAD4, NOTCH1, ERBB2&4, PIK3CA, MET, PTEN, EGFR, KRAS, BRAF and NRAS and were overlapping those of colorectal carcinoma. The study supports the possible use of genetic profiling and targeted therapy along lines of colorectal cancer.


八、对切除胆囊癌的新的体细胞改变的分子分析
背景:胆囊癌GBC常发现于晚期,预后不佳。对于GBC的分子特征研究还很有限。我们的研究机构使用了SEMA4实体肿瘤panel,对161个最相关的癌症驱动因子进行二代测序。我们报告了通过SEMA4panel确定的几个GBC中新的分子突变。
设计:SEMA4实体肿瘤panel被用于治疗了10例手术切除的GBC病例。分别记录人口统计、肿瘤大小、分级、分期和组织学亚型。分子研究结果和已发表的数据进行比较。
结果:我们检测了10例GBC患者,通过SEMA4对其进行分子分析(男性5例,女性5例,中位年龄68岁)。肿瘤平均大小2.2cm,良性2例,中分化6例,差分化2例,其中pT1 2例,pT2 6例,pT3 2例。组织学亚型上有8例未见明显特异,1例有粘液性表现,1例有印戒细胞特征。总体来看,42个体细胞突变包含34个基因被检测到。在这些突变中,在22个基因中的28个变异属于Tier1或Tier2改变,在治疗、预后和诊断方面具有很强的临床意义,而14例是Tier3,在一般或特殊的数据库中观察到显著的等位基因频率。平均检测的突变数与患者比值为4.4(Tier1/2 3.0,Tier3 1.4,整体范围1-11)。
在7例病例中检测到TP53突变(6个不同变异),MDM2扩增2例,ARID1A SNVS 2例,与已公布的频率相似,但6例TP53变异中有4例未在GBC中报道过。其他每个改变可以1名患者中见到。我们发现了RHOA和CDK2基因改变,以前从未在GBC病例中报道过。在ATR, BAP1, NOTCH1, SETD2, CTNNB1, PIK3R1, PIK3CA,EGFR发现了新的Tier1/2变异,在ARID1A, ATXR, CHEK1, RAD51C, FANCA, NOTCH 3, SETD2, SMARCB1, PIK3CB, NF1, ESR1发现了Tier3变异。通过Cytoscape,一种可视化分子相互作用网络的生物信息平台,初步分析强调了ERBB,PI3K和RAS信号,非RTK信号的激活和DNA损伤反应。
结论:我们的研究发现几种新的可能对于胆囊癌预后有重要意义的基因变化。这些发现的验证可能作用于潜在的靶向治疗,以改善这些毁灭性肿瘤患者的预后。
8.Molecular Analysis Reveals Novel Somatic Alterations in Resected Gallbladder Carcinomas
(Zhen Zhao, Stephen Ward)
Background: Gallbladder cancer (GBC) often presents at an advanced stage and has a dismal prognosis. Molecular characterization of GBC has thus far been limited. Our institution utilizes the SEMA4 solid tumor panel, a next generation sequencing analysis of 161 of the most relevant cancer drivers. We report several novel molecular alterations in GBC from our institution identified by the SEMA4 panel.
Design: SEMA4 solid tumor panel was applied to 10 cases of surgically resected GBC. Demographics, tumor size, grade, stage, and histologic subtype were recorded. Molecular findings were compared with existing published data.
Results: We identified 10 patients with GBC that underwent molecular analysis by SEMA4 (5 male, 5 female, median age 68 years). Mean tumor size was 2.2 cm, 2 were well-, 6 were moderately-, and 2 were poorly-differentiated while 2 were pT1, 6 were pT2 and 2 were pT3. The histologic subtype was not otherwise specified in 8 and mucinous in 1, while 1 had signet ring cell features. Overall, 42 somatic genetic alterations involving 34 genes were identified. Of these, 28 variants in 22 genes were Tier 1 or Tier 2 changes with strong or potential clinical significance of therapeutic, prognostic and diagnostic actionability, while 14 were Tier 3, yet observed at a significant allele frequency in the general or specific databases. The average detected alteration number/patient was 4.4 (3.0 Tier 1/2, 1.4 Tier 3; overall range 1-11).
TP53 mutation was seen in 7 cases (6 different variants), MDM2 amplification in 2, and ARID1A SNVs in 2, similar to published frequencies, though 4 of the 6 TP53 variants have not been previously reported in GBC. All other alterations were seen in 1 patient each. We found alterations in RHOA and CDK2, previously not reported in GBC. Novel Tier 1/2 alterations were seen in ATR, BAP1, NOTCH1, SETD2, CTNNB1, PIK3R1, PIK3CA and EGFR, and novel Tier 3 variants of ARID1A, ATXR, CHEK1, RAD51C, FANCA, NOTCH 3, SETD2, SMARCB1, PIK3CB, NF1, and ESR1 were identified. Using Cytoscape, an open-source bioinformatics platform for visualizing molecular interaction networks, preliminary analysis highlights activation of ERBB, PI3K and Ras signaling, non-RTK signaling, and impaired DNA damage response.
Conclusions: Our work highlights several new genetic alterations that may be important in the pathogenesis of GBC. Validation of these findings may lead to potential targeted therapies and improved patient outcomes for these devastating tumors.
翻译者:王语林
本文转载自复旦大学附属中山医院分子病理中心洞见分子
不感兴趣
看过了
取消

人点赞

人收藏

打赏
不感兴趣
看过了
取消
©2012-2023 北京华媒康讯信息技术股份有限公司 All Rights Reserved. 注册地址:北京 联系电话:010-82736610
广播电视节目制作经营许可证 —(京)字第 17437号 京海食药监械经营备20200522号
京ICP备12011723号 京ICP证150092号
 京公网安备 11010802020745号
工商备案公示信息
互联网药品信息服务资格证书((京)-非经营性-2020-0015)
京公网安备 11010802020745号
工商备案公示信息
互联网药品信息服务资格证书((京)-非经营性-2020-0015)






您已认证成功,可享专属会员优惠,买1年送3个月!
开通会员,资料、课程、直播、报告等海量内容免费看!

打赏金额
认可我就打赏我~
1元 5元 10元 20元 50元 其它
打赏作者
认可我就打赏我~
扫描二维码
立即打赏给Ta吧!
温馨提示:仅支持微信支付!
已收到您的咨询诉求 我们会尽快联系您
































 010-82736610
010-82736610
 股票代码: 872612
股票代码: 872612




