


















CSCO丨小细胞肺癌诊疗指南(2020)









【注释】
1. 小细胞肺癌(small cell lung cancer,SCLC)异质性、侵袭性强,诊治过程中更应重视多学科 团队(multidisciplinary team,MDT) 的作用,推荐有条件的单位尽可能进行 SCLC 的 MDT, 对患者进行全程管理。
2. MDT 的实施过程中需由多个学科的专家共同分析患者的病史、临床表现、影像学、病理学和 分子生物学资料,并对患者的一般状况、疾病的诊断、分期、发展趋势和预后做出全面的评估, 并根据当前国内外的治疗指南 / 规范和高级别的循证医学证据,结合目前可及的治疗手段和患 者的治疗意愿,为患者制订个体化的整体治疗策略。
3. MDT 团队可根据治疗过程中患者体能状态的变化和治疗疗效适时调整治疗方案,目的是最大 化的延长患者的生存期、提高治愈率和改善生活质量。


【注释】
1. 筛查
肺癌是中国和全球范围内发病率和病死率较高的恶性肿瘤,其中 SCLC占肺癌的 13%~17%[1]。由于 SCLC恶性程度高,早期极易发生远处转移,确诊时多为晚期,预后极差。而早期发现是延长SCLC患者生存期的有效方法,但目前尚无专门针对SCLC筛查的临床试验,多为肺癌高危人群的筛查研究。美国国家肺癌筛查试验(National Lung Screening Trial,NLST) 纳入了 53 454 名重度吸烟患者进行随机对照研究,评估采用低剂量螺旋CT筛查肺癌的获益和风险[2],结 果提示与胸片相比,低剂量螺旋CT筛查的高危人群,肺癌相关死亡率降低了 20%(95%CI 6.8~26.7;P =0.004)[3],其中 SCLC 占比 8%;其他较大的肺癌筛查试验诊断的肺癌患者中,SCLC 的比例为 4%~9%[4]。
2. 诊断与分期
胸部增强 CT、腹部、盆腔增强 CT、头部增强 MRI 或增强 CT 及全身骨显像是 SCLC 分期 和诊断的主要方法。FDG-PET-CT 对分期诊断有较好的效能,近期数据显示[5]PET-CT可以改善SCLC患者的分期和治疗计划;另外有临床试验和随机对照研究发现[6-8],肺癌患者通过FDG- PET-CT 扫描可以降低 17%~20% 的开胸率。但由于 PET-CT 价格昂贵,故仅作为Ⅱ级推荐;SCLC诊断时脑转移的发生率为 10%~18%,其中,将近30%的患者无脑转移相关症状,PET-CT 在发现脑转移方面不如MRI或者CT。Tatjana Seute 等对比了不同时期481名SCLC患者脑转移发生的流行病学数据[9],发现在 CT 时期 SCLC 脑转移的发生率为 10%,而核磁时期发生率高达24%, 其中11% 的患者为无症状脑转移,并且多发脑转移的检出率也明显增高。当纵隔淋巴结或浆膜腔 积液影响治疗决策,而现有手段又难以确认时,推荐 EBUS、浆膜腔积液穿刺等有创手段明确纵 隔淋巴结或浆膜腔积液性质;痰细胞学由于容易产生诊断错误,在组织学检查可行的情况下,应减少痰细胞学的应用。
3. 分期方法
SCLC 的分期一直沿袭美国退伍军人肺癌协会(VALG) 的二期分期法[10],主要基于放疗在SCLC治疗中的重要地位。AJCC TNM分期系统可以选出适合外科手术的 T1-2N0M0 的局限期患者, 能更准确地了解患者所处的疾病阶段、判断患者的预后及制订合适的治疗方案[11,12]。建议临床使用 VALG 分期法和 TNM 分期系统两者相结合的方法对 SCLC 进行分期,因其更能准确地指导治疗 和评估预后[5,13]。
(1)VALG 二期分期法:
局限期:病变限于一侧胸腔,且能被纳入一个放射治疗野内。
广泛期:病变超过一侧胸腔,且包括恶性胸腔和心包积液或血行转移。
(2)NCCN 治疗小组建议 SCLC 分期采取 AJCC TNM 分期方法与 VALG 二期分期法相结合:局限期:AJCC(第 8 版)Ⅰ~ Ⅲ期(任何 T,任何 N,M0),可以安全使用根治性的放疗剂量。排除 T3-4 由于肺部多发结节或者肿瘤 / 结节体积过大而不能被包含在一个可耐受的放疗计划中。
广泛期:AJCC(第 8 版) Ⅳ期(任何 T,任何 N,M1a/b/c),或者 T3-4 由于肺部多发结节或者肿瘤 / 结节体积过大而不能被包含在一个可耐受的放疗计划中。
参考文献
[1]ORONSKY B, REID T R, ORONSKY A, et al. What’s new in SCLC ?A review [J] . Neopla- sia, 2017, 19 (10): 842-847.
[2]ABERLE D R, BERG C D, BLACK W C, et al. The national lung screening trial: overview and study
design [J] . International Journal of Medical Radiology, 2011, 258 (1): 243-253.
[3]ABERLE D R, ADAMS A M, et al. None. Reduced Lung-Cancer Mortality with Low-Dose Computed Tomographic Screening [J] . New England Journal of Medicine, 2011, 365 (5): 395-409.
[4]VANDAC M, TEN HAAF K, De KONING H J. Lung cancer screening: latest developments and unan-
swered questions [J] . The Lancet Respiratory Medicine, 2016, 4 (9): 749-761.
[5]GREGORY P. KALEMKERIA N, SHIRISH M, et al. Modern staging of small cell lung can- cer [J] . Journal of the National Comprehensive Cancer Network, 2013, 11 (1): 99-104.
[6]FISCHER B, LASSEN U, MORTENSEN J, et al. Preoperative staging of lung cancer with combined PET-CT [J] . N Engl J Med, 2009, 361 (1): 32-39.
[7]REED C E, HARPOLE D H, POSTHER K E, et al. Results of the American College of Surgeons Oncology Group Z0050 trial: the utility of positron emission tomography in staging potentially Oper- able non-small cell lung cancer [J] . J Thorac Cardiovasc Surg, 2003, 126 (6): 1943-1951.
[8]VAN TINTEREN H, HOEKSTRA O S, SMIT E F, et al. Effectiveness of positron emission tomography in the preoperative assessment of patients with suspected non-small-cell lung cancer: the PLUS multicentre randomized trial [J] . Lancet, 2002, 359 (9315): 1388-1393.
[9] SEUTE T, LEFFERS P, TEN VELDE G P M, et al. Detection of brain metastases from small cell lung cancer: consequences of changing imaging techniques (CT versus MRI) [J] . Can- cer, 2008, 112 (8): 1827-1834.
[10]MICKE P, FALDUM A, METZ T, et al. Staging small cell lung cancer: Veterans Administration Lung Study Group versus International Association for the Study of Lung Cancer—what limits limited dis- ease ?[J] Lung Cancer, 2002, 37 (3): 271-276.
[11]AMIN M B, GREENE F L, BYRD D R, et al. AJCC Cancer Staging Manual. 8th edi- tion [M] . Springer International Publishing, 2016.
[12]NICHOLSON A G, CHANSKY K, CROWLEY J, et al. The International Association for the Study of Lung Cancer lung cancer staging project: proposals for the revision of the clinical and pathologic staging of small cell lung cancer in the forthcoming eighth edition of the TNM classification for lung cancer [J] . J Thorac Oncol, 2016, 11 (3): 300-311.
[13]JETT J R, SCHILD S E, KESLER K A, et al. Treatment of small cell lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines [J] . Chest, 2013, 143 (5 Suppl): e400S-419S.




【注释】
细胞学标本诊断原则
1. 细胞学的标本来源主要包括气管镜刷检、浆膜腔积液、细针穿刺、痰及支气管灌洗等。
2. 根据肿瘤细胞的大小及形态,小细胞癌细胞学镜下可分为燕麦细胞型和中间细胞型:
(1)燕麦细胞型通常体积较小,可呈圆形、卵圆形、短梭形及长型,胞浆少或无,大小为静止期淋巴细胞的1.5~3 倍,在同一张涂片中肿瘤细胞大小较一致,也可见紧密巢状聚集,两种形态可同时出现于一张涂片中;核染色质呈均匀细颗粒状,可见染色质集结点,也可由 于细胞退化而导致染色质呈固缩状,通常较少见到明显核仁;相邻肿瘤细胞贴边镶嵌状排 列,制片过程中易出现核拉丝现象,但这种现象一般不在液基制片中出现。
(2)中间细胞型的肿瘤细胞排列及核特征与燕麦细胞型相似,肿瘤细胞可呈圆形、卵圆形、短 梭形或多角形等;核染色质也可呈粗颗粒状,胞浆可相对较丰富,同一张涂片中肿瘤细胞 胞浆可多可少甚至裸核,形态不规则,核分裂较多。
3. 对于浆膜腔积液和细针吸取标本,细胞学蜡块切片中肿瘤细胞的镜下形态与组织学相似,可见 由小的圆形、卵圆形或梭形的裸核样细胞聚集成巢或弥散分布,也可出现“人工挤压”现象。免疫细胞化学抗体选择与组织学基本相同,常用的抗体包括 TTF1、CD56、Syn、CgA、Ki-67、 CK 等。
组织标本诊断原则
1. 2015版WHO肺肿瘤分类将神经内分泌肿瘤分为 4 类,小细胞癌与大细胞神经内分泌癌属于高 级别肿瘤,典型类癌与不典型类癌属于低 - 中级别肿瘤。因此鉴别小细胞癌与其他神经内分泌 肿瘤,特别是典型和不典型类癌在流行病学、遗传学、治疗及预后等方面具有重要意义[3-5]。
2. 神经内分泌肿瘤标记物包括 CD56、Syn、CgA,在具有神经内分泌肿瘤形态学特征的基础上至少有一种神经内分泌免疫组化标记物明确阳性,且神经内分泌标记阳性的细胞数应大于 10% 肿 瘤细胞量才可诊断神经内分泌肿瘤。TTF-1 在 85%~90% 的小细胞肺癌中呈阳性表达[6~9]。当 少数小细胞肺癌病例中不表达神经内分泌标记物时,结合形态、TTF-1 弥漫阳性、CK 核旁点 状阳性颗粒特点及高 Ki-67 指数(一般为 50%~100%) 也有助于小细胞癌的诊断[1]。
3. 依据 2015 版 WHO 肺癌神经内分泌肿瘤分类标准,Ki-67 阳性指数目前还无法用来鉴别典型类 癌及不典型类癌,但在小活检标本中建议增加 Ki-67 检测,以防止将伴有机械性损伤的类癌、 不典型类癌诊断为小细胞肺癌。
4. 复合型小细胞肺癌为小细胞肺癌同时伴有其他任何非小细胞肺癌成分,如腺癌、鳞状细胞癌、
大细胞神经内分泌癌等。除大细胞神经内分泌癌需满足至少 10% 的比例外,其他非小细胞肺 癌类型可以是任何比例。
5. 如果同时有细胞学标本及活检标本时,应将两者结合进行考量,综合做出更恰当的诊断。
6. 手术标本怀疑肿瘤累及胸膜时,应进行弹力纤维特殊染色辅助诊断[10~11]。
7. 同一患者治疗后不同时间小标本活检病理诊断应尽量避免使用组织类型之间转化的诊断[12],
此种情况不能除外小活检标本取材受限,未能全面反映原肿瘤组织学类型,有可能原肿瘤是复 合型小细胞肺癌,化疗后可致其中非小细胞癌成分残留。
参考文献
[1]TRAVIS W D, BRAMBILLA E, BURKE A, et al. WHO Classification of Tumours of the Lung Pleura Thymus and Heart [M] . Lyon: IARC Press, 2015.
[2]TRAVIS W D. Advances in neuroendocrine lung tumors [J] . Ann Oncol, 2010, 21 (Suppl 7): vii65-71.
[3]PELOSI G, RODRIGUEZ J, VIALE G, et al. Typical and atypical pulmonary carcinoid tumor overdi- agnosed as small-cell carcinoma on biopsy spcimens: a major pitfall in the management of lung cancer patients [J] . Am J Surg Pathol, 2005, 29 (2): 179-187.
[4]PELOSI G, RINDI G, TRAVIS W D, et al. Ki-67 antigen in lung neuroendocrine tumors: unraveling a role in clinical practice [J] . J Thorac Oncol, 2014, 9 (3): 273-284.
[5]RINDI G, KLERSY C, INZANI F, et al. Grading the neuroendocrine tumors of the lung: an evidence- based proposal [J] . Endocr Relat Cancer, 2014, 21 (1): 1-16.
[6]ORDONEZ N G. Value of thyroid transcription factor-1 immunostaining in distinguishing small cell lung carcinomas form other small cell carcinomas [J] . Am J Surg Pathol, 2000, 24 (9): 1217-1223.
[7]KAUFMANN O, DIETEL M. Expression of thyroid transcription factor-1 in pulmonary and extrapul- monary small cell carcinomas and other neuroendocrine carcinomas of various primary sites [J] . His- topathology, 2000, 36 (5): 415-420.
[8]LANTUEJOUL S, MORO D, MICHALIDES R J, et al. Neural cell adhesion molecules (NCAM) and NCAM-PSA expression in neuroendocrine lung tumors [J] . Am J Surg Pathol, 1998, 22 (10): 1267- 1276.
[9]WICK M R. Immunohistology of neuroendocrine and neuroectodermal tumors [J] . Semin Diagn Pathol, 2000, 17 (3): 194-203.
[10]BUTNOR K J, BEASLEY M B, CAGLE P T, et al. Protocol for the examination of specimens form patients with primary non-small cell carcinoma, small cell carcinoma, or carcinoid tumor of the lung [J] . Arch Pathol Lab Med, 2009, 133 (10): 1552-1559.
[11]TRAVIS W D, BRAMBILLA E, RAMI-PROTA R, et al. Visceral pleural invasion; pathologic criteria and use of elastic stains: proposal for the 7th edition of the TNM classification for lung cancer [J] . J Thorac Oncol, 2008, 3 (12): 1384-1390.
[12]HASLETON P, FLIEDER D B. Spencer‘s Pathology of the Lung. 6th ed [M] . Cambridge University Press, 2013.


【注释】
1. 胃泌素释放肽前体(precursor of Gastrin-Releasing Peptide,proGRP) 和神经元特异性烯醇化酶(neuron specific enolase,NSE)是 SCLC 诊断以及治疗效果监测的重要肿瘤标志物。研究证实,胃泌素释放肽是 SCLC 组织的重要产物,其在血清里的前体可被稳定检测。SCLC 可表现为神 经内分泌细胞的特性,因此 NSE 往往会有过量表达。联合检测 proGPR 和 NSE 可以提高 SCLC 的诊断率,在局限期 SCLC 治疗有效的情况下,这两个值会随之下降[2-4]。
2. 肿瘤突变负荷(tumor mutation burden,TMB) 可能预测免疫检查点抑制剂疗效,利用 NGS 多基因组合估测 TMB 是临床可行的方法[5]。免疫治疗在 SCLC 中已取得一定疗效。Ⅰ/ Ⅱ期 CheckMate032 研究证实,nivolumab + ipilimumab 治疗高 TMB 患者有效率可达 46.2%,1 年 PFS 率为 30.0%,显著优于低、中 TMB 亚组[6]。在组织标本不足时,利用 NGS 检测循环血肿 瘤细胞 DNA(ctDNA) 进行 TMB 估测是潜在可行的技术手段之一[7,8]。
3. 目前针对 SCLC 尚无批准的靶向药物或指导治疗的标志物。替莫唑胺(temozolomide)在 复发性 SCLC 中有一定的疗效,脑转移、MGMT(O6- 甲基鸟嘌呤 -DNA- 甲基转移 酶) 基 因甲基化阳性患者可能疗效更好[6,9,10]。国家 药品监督管理局(National Medical Products Administration,NMPA) 已于 2019 年批准人类 MGMT 基因甲基化检测试剂盒(荧光 PCR 法) 用于定性检测石蜡切片样本中 MGMT 的甲基化状态。
4. 在 SCLC 中,DNA 损伤修复相关基因(如 BRCA1/2) 突变并不常见,不能用来预测 PARP 抑 制剂疗效[11]。研究表明,PARP 依赖的碱基剪切修复是替莫唑胺耐药重要机制之一[12],替莫 唑胺联合 PARP 抑制剂 veliparib 与替莫唑胺联合安慰剂相比,虽然未能明显延长 PFS 和 OS, 但显著提高了 SCLC 患者 ORR(39% vs 14%,P=0.016)。Schlafen-11(SLFN11) 调控 DNA 损 伤应答和复制应激,可在多种癌症中预测 DNA 损伤机制,化疗药物[13]和 PARP 抑制剂敏感性[11,14,15]。SLFN11 蛋白表达与替莫唑胺联合 veliparib 治疗患者的 PFS 和 OS 显著相关,有 望成为 PARP 抑制剂治疗 SCLC 疗效的预测标志物[9]。
5. 循环肿瘤细胞(circulating tumor cells,CTCs) 是指在循环血液中存在的具有肿瘤特征的细胞。CTCs 作为一种代表原发肿瘤的“液态活检标本”,可实时、动态地、无创性地对 SCLC 患者病 情进行监测。研究证实 SCLC 细胞分裂周期短、增殖快,易进入血液循环继而发生远处转移, CTCs 在 SCLC 人群中检出率为 67%~86%,检测 CTCs 有助于正确判断疾病临床分期,以便选 择合适的治疗方案、指导 SCLC 患者的个体化治疗、监测肿瘤复发与转移、判定治疗疗效及预 测预后生存,同时也是分析耐药分子机制及解决肿瘤异质性的一种手段[16~22]。
6. 对于混有 NSCLC 成分的复合型 SCLC,推荐不吸烟的广泛期患者进行分子检测,以协助明确 诊断和评估潜在的靶向治疗方案。
参考文献
[1]HELLMANN M, CIULEANU T E, PLUZANSKI A, et al. Nivolumab plus ipilimumab in lung cancer with a high tumor mutational Burden [J] . N Engl J Med, 2018, 378 (22): 2093-2104.
[2]SHIBAYAMA H U, NISHII K E, KIURA K A, et al. Complementary roles of pro-gastrin-releasing peptide (ProGRP) and neuron specific enolase (NSE) in diagnosis and prognosis of small-cell lung cancer (SCLC) [J] . Lung Cancer, 2001, 32 (1): 61-69.
[3] WÓJCIK K, SAS-KORCZY SKA B, KORZENIOWSKI S, et al. ProGRP and NSE in therapy moni- toring in patients with small cell lung cancer [J] . Anticancer Res, 2008, 28 (5B): 3027-3034.
[4]WOJCIK E, KULPA J, SAS-KORCZYNSKA B. ProGRP and NSE for follow-up of small cell lung cancer patients with limited disease [J] . Journal of Thoracic Oncology, 2007: 2061.
[5]SAMSTEIN R M, LEE C H, SHOUSHTARI A N, et al. Tumor mutational load predicts survival after immunotherapy across multiple cancer types [J] . Nat Genet, 2019, 51 (2): 202-206.
[6]PIETANZA M C, KADOTA K, HUBERMAN K, et al. Phase Ⅱtrial of temozolomide in patients with relapsed sensitive or refractory small cell lung cancer, with assessment of methylguanine-DNA meth- yltransferase as a potential biomarker. Clin Cancer Res, 2012, 18 (4): 1138-1145.
[7]WANG Z, DUAN J, CAI S, et al. Assessment of blood tumor mutational burden as a potential bio- marker for immunotherapy in patients with non-small cell lung cancer with use of a next-generation sequencing cancer gene panel [J] . JAMA Oncol, 2019, 5 (5): 696-702.
[8]GANDARA D R, PAUL S M, KOWANETZ M, et al. Blood-based tumor mutational burden as a predictor of clinical benefit in non-small-cell lung cancer patients treated with atezolizumab [J] . Nat Med, 2018, 24 (9): 1441-1448.
[9]PIETANZA M C, WAQAR S N, KRUG L M, et al. Randomized, double-blind, phase ii study of temo- zolomide in combination with either veliparib or placebo in patients with relapsed-sensitive or refrac-tory small-cell lung cancer [J] . J Clin Oncol, 2018, 36 (23): 2386-2394.
[10]ZAUDERER M G, DRILON A, KADOTA K, et al. Trial of a 5-day dosing regimen of temozolomide in patients with relapsed small cell lung cancers with assessment of methylguanine-DNA methyl- transferase [J] . Lung Cancer, 2014, 86 (2): 237-240.
[11]ALLISON C, TONG P, CARDNELL R J, et al. Dynamic variations in epithelial-to-mesenchymal transition (EMT) , ATM, and SLFN11 govern response to PARP inhibitors and cisplatin in small cell lung cancer [J] . Oncotarget, 2017, 8 (17): 28575-28587.
[12]MURAI J, TANG S W, LEO E, et al. SLFN11 blocks stressed replication forks independently of ATR [J] . Mol Cell, 2018, 69 (3): 371-384.
[13]ZOPPOLI G, REGAIRAZ M, LEO E, et al. Putative DNA/RNA helicase Schlafen-11 (SLFN11) sen- sitizes cancer cells to DNA-damaging agents [J] . Proc Natl Acad Sci U S A, 2012, 109 (37): 15030- 15035.
[14]LOK B H, GARDNER E E, SCHNEEBERGER V E, et al. PARP inhibitor activity correlates with SLFN11 expression and demonstrates synergy with temozolomide in small cell lung cancer [J] . Clin Cancer Res, 2017, 23 (2): 523-535.
[15 ]POLLEY E, KUNKEL M, EVANS D, et al. Small cell lung cancer screen of oncology drugs, investi- gational agents, and gene and microRNA expression [J] . J Natl Cancer Inst, 2016, 108 (10) .
[16]CHENG Y, LIU X Q, FAN Y, et al. Circulating tumor cell counts/change for outcome prediction in patients with extensive-stage small-cell lung cancer [J] . Future Oncol, 2016, 12 (6): 789-799.
[17]NORMANNO N, ROSSI A, MORABITO A, et al. Prognostic value of circulating tumor cells’ reduction in patients with extensive small-cell lung cancer. Lung Cancer, 2014, 85 (2): 314- 319.
[18]HOU JM, KREBS M G, LANCASHIRE L, et al. Clinical significance and molecular characteristics of circulating tumor cells and circulating tumor microemboli in patients with small-cell lung can- cer [J] . J Clin Oncol, 2012, 30 (5): 525-532.
[19]HILTERMANN T J, PORE M M, VAN A, et al. Circulating tumor cells in small-cell lung cancer: a predictive and prognostic factor [J] . Ann Oncol, 2012, 23: 2937-2942.
[20]NAITO T, TANAKA F, ONO A, et al. Prognostic impact of circulating tumor cells in patients with small cell lung cancer. J Thorac Oncol, 2012, 7 (3): 512-519.
[21]AGGERWAL C H, WANG X M, RANGANATHAN A N, et al. Circulating tumor cells as a predic- tive biomarker in patients with small cell lung cancer undergoing chemotherapy [J] . Lung Can- cer, 2017, 112: 118-125.
[22]TAY R Y, FERNA F, RREZ N D, et al. Prognostic value of circulating tumour cells in limited-stage small-cell lung cancer: analysis of the concurrent once-daily versus twice-daily radiotherapy (CON- VERT) randomised controlled trial [J] . Ann Oncol, 2019, 30 (7): 1114-1120.


【注释】
1. 局限期 SCLC 手术治疗
临床分期为Ⅰ~ ⅡA 期的患者术前应行病理性纵隔分期,包括纵隔镜检查、纵隔切开术、经气 管或者经食管的超声(EBUS) 引导下活检以及电视胸腔镜检查等。若内镜下淋巴结活检是阳性的, 不需要其他纵隔分期检查。如果患者不适合手术或者不希望手术治疗,不需进行病理纵隔分期。对 SCLC,PET-CT 是比常规影像检查更好的分期手段,据报道常规影像方法分期为局限期的患者经 PET-CT 检查有 19% 的患者变为广泛期,也有 8% 的广泛期 SCLC 转为局限。
Ⅰ~ ⅡA 期的 SCLC 可能从手术中获益。现有的数据显示,手术组和非手术组患者 5 年生存率 范围分别在 27%~73% 和 4%~44%。Yang[17]等基于 NCDB 数据库的倾向匹配分析中发现,手术治 疗能显著改善 5 年的生存率(47.6% 和 29.8%,P<0.01)。手术方式方面,多项回顾性研究和荟萃分 析[17,18]的亚组分析均显示,肺叶切除组的生存优于楔形切除。
ⅡB~ ⅢA 期 SCLC,手术的作用存在争议。尽管一些回顾性研究获得了阳性结果,但这些研究 中已经获得的中位生存期范围为 17~31.7 个月,与同步放化疗的 CONVERT 研究[19]的 25 个月相比 并未有突破性的提升,故手术对于ⅡB~ ⅢA 期小细胞肺癌的有效性及适合亚群仍待商榷。ⅢB~ ⅢC 期 SCLC,缺乏有效证据证明手术有效,因此不推荐接受手术治疗。
2. 局限 SCLC 胸部放疗
(1)辅助放疗:研究发现,术后 N2 患者辅助放疗能够提高 OS(22 个月 vs 16 个月)[5],因此推荐术后 N2 患者接受辅助放疗。一项基于 NCDB 的回顾性分析显示,与未行辅助放疗 相比,N1 患者辅助胸部放疗的 5 年生存率在数值上提高 5.6%,但没有获得统计学上显著 差异(P=0.22),基于两组样本量不均衡,缺少局部复发的数据,建议术后 N1 的患者进 行辅助放疗[6],同步或序贯均可[20-22]。目前辅助放疗推荐采用三维适形技术(3D-CRT)、 调强技术(IMRT) 或容积旋转调强技术(VMAT),靶区主要包括同侧肺门、同侧纵隔和 隆突下等局部复发高危区域,总剂量 50Gy。
(2)不适宜手术或拒绝行手术的 I~ ⅡA 期 SCLC:除了同步放化疗外,对原发肿瘤行 SBRT/ SABR,然后进行全身化疗是可选择的治疗。SBRT/SABR 的治疗原则同非小细胞肺癌。SBRT/SABR 生物学等效剂量≥ 100Gy可以取得更好的局部控制和生存率 [23],RTOG 0813 研究显示 50Gy/5f 没有发生严重的毒性反应[24]。对于 SBRT/SABR 设备要求:要具 备 IGRT 功能,TPS 支持多模态图像(融合) 和复杂设计计划功能。应用 SBRT/SABR 时 能够应用 CT/4D-CT 模拟定位精确勾画定位 CT 图像,扫描层厚:1~3mm,通过慢速 CT、 屏气技术、门控技术、4D-CT 等实现对运动靶区数据的获取和呼吸运动的管理。MLC 的宽度要求在 5mm 以下。建议用≤ 2.0mm 的计算网格。对于治疗中的影像引导需要有 CBCT 配准、体内标记、体表标记及追踪技术支持。用于做 SBRT/SABR 的设备各项参 数精度如等中心、激光灯、图像引导、图像质量等,要高于常规 IMRT 治疗所用设备的 要求。
(3)超过T1-2N0 的局限期 SCLC 患者,同步放化疗为标准治疗。如果患者不能耐受,也可行序贯化放疗。经Ⅲ期随机对照研究验证,实行同步放化疗优于序贯放化疗[10]。加拿大一 项研究比较在化疗第 2 与第 6 周期开始放疗的疗效,发现早期放疗可提高局部和全身控制 率,获得更长的生存期[25]。所以胸部放疗应在化疗的第 1~2 个周期尽早介入[26,27],对 于特殊的临床情况,如肿瘤巨大、合并肺功能损害、阻塞性肺不张等,可考虑 2 个周期化 疗后进行放疗。同步化疗方案推荐使用顺铂 / 依托泊苷,每周期 21~28 天。
(4)放疗总剂量和分割方案:目前尚未确定最佳的放疗剂量和分割方案。根据 INT 0096 研究, 45Gy/1.5Gy,b.i.d./3 周方案优于 45Gy,1.8Gy,q.d./5 周方案[11,12]。而 CONVERT 研究 未能证明 66Gy(每天 1 次) 方案优于 45 Gy(b.i.d.) 方案,两组的总生存率和毒性均相 似[34],推荐局限期 SCLC 患者胸部放疗总剂量为 45Gy/1.5Gy,b.i.d./3 周[11,12]或总剂量 为 60~70Gy,1.8~2.0Gy,q.d./6~8 周[14]。
(5)放疗靶区:靶区勾画原则为原发灶靶区应按照化疗后残留肿瘤勾画,对于诱导化疗后完全 缓解的淋巴结,也应该照射淋巴结所在的整个引流区,有明确的纵隔淋巴结转移者,即使 同侧肺门未发现肿大淋巴结,靶区包括同侧肺门也是合理的。一项前瞻性非劣效性随机对 照研究中,化疗前和化疗后肿瘤范围进行放疗的局部复发率、孤立性淋巴结失败率和 OS 均无显著性差异[28]。放疗至少要采用 CT 模拟定位和三维适形技术。当需要达到足够的 肿瘤剂量而又要顾及正常组织的限量时,则需要采用更先进的技术,包括(但不仅限于):四维 CT(4DCT)和 / 或 PET-CT 模拟定位,IMRT/VMAT,图像引导放疗技术(IGRT) 以及呼吸门控技术。
3. 局限期 SCLC 的 PCI
局限期 SCLC,前期经过根治性化疗和胸部放疗,获得较好的疗效(PR/CR) 的患者,行 PCI, 可以降低颅内转移的概率并提高整体生存率[2]。而接受根治性手术和系统化疗的Ⅰ期 SCLC 患者, 因为后期发生的脑转移率较低(<10%),脑预防放疗可能获益较低[29]。全脑预防放疗的剂量建议为 25Gy/10 次。开始时机建议完成放化疗治疗后 3~4 周。具体的放疗技术可选择常规放疗,适形放疗, 有条件的前提下推荐海马保护的调强放疗(IMRT)[30]。对于高龄(大于 65 岁),PS>2,有神经认 知功能受损的患者不建议行 PCI。
4. 局限期 SCLC 的内科治疗
(1)依托泊苷联合铂类是局限期 SCLC 一线治疗的经典方案。荟萃分析比较了 SCLC 患者采用 顺铂为基础和卡铂为基础的方案,两组 ORR 无差异(67% vs 66%),PFS 和 OS 也无差异
(分别为 5.5 个月 vs 5.3 个月;9.6 个月 vs9.4 个月),证实顺铂和卡铂方案在 SCLC 中疗效 相似[9]。
(2)术后辅助化疗:术后均应接受含铂辅助化疗[32,33]。NCDB 数据库分析显示,对于 pT1- 2N0M0 的患者,辅助化疗(无论是否联合放疗) 能够降低 22% 的死亡风险(HR= 0.78,
95%CI 0.63~0.95)[33]。辅助化疗采用 EP 或 EC 方案。
(3) PS 评分 3~4 的局限期 SCLC 患者,治疗上大体分为以下两种情况:①如果为 SCLC 所致, 应充分综合考虑各种因素,谨慎选择治疗方案,如化疗(单药方案或减量联合方案),如 果治疗后 PS 评分能达到 0~2,可考虑给予同步或序贯放疗;如果 PS 评分仍无法恢复至2 分以上,则根据具体情况决定是否采用胸部放疗。②如果为非 SCLC 所致,经对症支持 治疗后,如果体力状况得到改善,PS 评分能够达到 0~2 分,可按照 PS 0~2 组患者的治疗 策略进行治疗。
(4)对于老年 SCLC 患者,不能仅根据年龄确定治疗方案,根据机体功能状态指导治疗更有意 义。如果老年患者日常生活自理能力、体力状况良好、器官功能相对较好,应当接受标准 联合化疗(如果有指征也可放疗),但因老年患者可能有更高的概率出现骨髓抑制、乏力 和器官功能储备较差,所以在治疗过程中应谨慎观察,以避免过高的风险。
参考文献
[1]LAD T, PIANTADOSI S, THOMAS P, et al. A prospective randomized trial to determine the benefit of surgical resection of residual disease following response of small cell lung cancer to combination che- motherapy [J] . Chest, 1994, 106 (6 Suppl): 320S-323S.
[2]AUPERIN A, ARRIAGADA R, PIGNON J P, et al. Prophylactic cranial irradiation for patients with small-cell cancer in complete remission. Prophylactic Cranial Irradiation Overview Collaborative Group [J] . N Engl J Med, 1999, 341 (7): 476-484.
[3]SHEPHERD F A, EVANS W K, FELD R, et al. Adjuvant chemotherapy following surgical resection for small-cell carcinoma of the lung [J] . J Clin Oncol, 1988, 6 (5): 832-838.
[4]TSUCHIYA R, SUZUKI K, ICHINOSE Y, et al. Phase Ⅱ trial of postoperative adjuvant cis- platin and etoposide in patients with completely resected stage Ⅰ - Ⅲ a small cell lung cancer: the Japan Clinical Oncology Lung Cancer Study Group Trial (JCOG9101) [J] . J Thorac Cardiovasc Surg, 2005, 129 (5): 977-983.
[5]SCHREIBER D, RINEER J, WEEDON J, et al. Survival outcomes with the use of surgery in limited- stage small cell lung cancer: should its role bere-evaluated ?[J] Cancer, 2010, 116 (5): 1350-1357.
[6]WONG A T, RINEER J, SCHWARTZ D, et al. Assessing the impact of postoperative radiation therapy for completely resected limited-stage small cell lung cancer using the national cancer database [J] . J Thorac Oncol, 2016, 11 (2): 242-248.
[7]TIMMERMAN R, PAULUS R, GALVIN J, et al. Stereotactic body radiation therapy for inoperable early stage lung cancer [J] . JAMA, 2010, 303 (11): 1070-1076.
[8]SUNDSTROM S, BREMNES R M, KAASA S, et al. Cisplatin and etoposide regimen is superior to cyclophosphamide, epirubicin, and vincristine regimen in small-cell lung cancer: results from a ran- domized phase Ⅲtrial with 5 years’follow-up [J] . J Clin Oncol, 2002, 20 (24): 4665-4672.
[9]ROSSI A, DI MAIO M, CHIODINI P, et al. Carboplatin-or cisplatin-based chemotherapy in first-line treatment of small-cell lung cancer: the COCIS meta-analysis of individual patient data [J] . J Clin Oncol, 2012, 30 (14): 1692-1698.
[10]TAKADA M, FUKUOKA M, KAWAHARA M, et al. Phase Ⅲ study of concurrent versus sequential thoracic radio therapy in combination with cisplatin and etoposide for limited-stage small-cell lung cancer: results of the Japan Clinical Oncology Group Study 9104 [J] . J Clin Oncol, 2002, 20 (14): 3054-3060.
[11]TURRISI A T, KIM K, BLUM R, et al. Twice-daily compared with once-daily thoracic radiotherapy in limited small-cell lung cancer treated concurrently with cisplatin and etoposide [J] . N Engl J Med, 1999, 340 (4): 265-271.
[12]SCHILD S E, BONNER J A, SHANAHAN T G, et al. Long-term results of a phase Ⅲ trial comparing once-daily radiotherapy with twice-daily radiotherapy in limited-stage small-cell lung cancer [J] . Int J Radiat Oncol Biol Phys, 2004, 59 (4): 943-951.
[13]CHOI N C, HERNDON J E, ROSENMAN J, et al. Phase I study to determine the maximum-tolerated dose of radiation in standard daily and hyperfractionated-accelerated twice-daily radia- tion schedules with concurrent chemotherapy for limited-stage small-cell lung cancer [J] . J Clin Oncol, 1998, 16 (11): 3528-3536.
[14]MILLER K L, MARKS L B, SIBLEY G S, et al. Routine use of approximately 60 Gy once-daily thoracic irradiation for patients with limited-stage small-cell lung cancer [J] . Int J Radiat Oncol Biol Phys, 2003, 56 (2): 355-359.
[15]ROOF K S, FIDIAS P, LYNCH T J, et al. Radiation dose escalation in limited-stage small-cell lung cancer [J] . Int J Radiat Oncol Biol Phys, 2003, 57 (3): 701-708.
[16]BOGART J A, HERNDON J E, LYSS A P, et al. 70 Gy thoracic radiotherapy is feasible concurrent with chemotherapy for limited-stage small-cell lung cancer: analysis of cancer and leukemia group B study 39808 [J] . Int J Radiat Oncol Biol Phys, 2004, 59 (2): 460-468.
[17]YANG C J, CHAN D Y, SHAH S A, et al. Long-term survival after surgery compared with concurrent chemoradiation for node-negative small cell lung cancer [J] . Ann Surg, 2018, 268 (6): 1105- 1112.
[18]LIU T, CHEN Z, DANG J, LI G. The role of surgery in stage Ⅰto Ⅲsmall cell lung cancer: A systematic review and meta-analysis [J] . PLoS One, 2018, 13 (12): e0210001.
[19]FAIVRE-FINN C, SNEE M, ASHCROFT L, et al. Concurrent once-daily versus twice-daily chemo- radiotherapy in patients with limited-stage small-cell lung cancer (CONVERT): an open-label, phase 3, randomised, superiority trial [J] . Lancet Oncol, 2017, 18 (8): 1116-1125.
[20]YANG C J, CHAN D Y, SPEICHER P J, et al. Surgery versus optimal medical management for small cell lung cancer [J] . Ann Thorac Surg, 2017, 103 (6): 1767-1772.
[21]URUSHIYAMA H, JO T, YASUUNAGA H, et al. Adjuvant chemotherapy versus chemoradiotherapy for small cell lung cancer with lymph node metastasis: a retrospective observational study with use of a national database in Japan [J] . BMC Cancer, 2017, 17 (1): 613.
[22]ZHANG S, SUN X, SU N, et al. Benefits of postoperative thoracic radiotherapy for small cell lung cancer subdivided by lymph node stage: a systematic review and meta-analysis [J] . J Thorac Dis, 2017, 9 (5): 1257-1264.
[23]ONISHI H, SHIRATO H, NAGATA Y, et al. Hypofractionated stereotactic radiotherapy (HypoFX-SRT) for stageⅠnon-small cell lung cancer: updated results of 257 patients in a Japanese multi- institutional study [J] . J Thorac Oncol, 2007, 2 (7 Suppl 3): S94-100.
[24]BEZJAK A, PAULUS R, GASPAR L E, et al. Safety and efficacy of a five-fraction stereotactic body radiotherapy schedule for centrally located non-small-cell lung cancer: NRG Oncology/RTOG 0813 Trial [J] . J Clin Oncol, 2019, 37 (15): 1316-1325.
[25]MURRAY N, COY P, PATER J L, et al. Importance of timing for thoracic irradiation in the combined modality treatment of limited-stage small-cell lung cancer. The National Cancer Institute of Canada Clinical Trials Group [J] . J Clin Oncol, 1993, 11 (2): 336-344.
[26] FRIED D B, MORRIS D E, POOLE C, et al. Systematic review evaluating the timing of thoracic radiation therapy in combined modality therapy for limited-stage small-cell lung cancer [J] . J Clin Oncol, 2004, 22 (23): 4837-4845.
[27]STINCHCOMBE T E, GORE E M. Limited-stage small cell lung cancer: current chemoradiotherapy treatment paradigms [J] . Oncologist, 2010, 15 (2): 187-195.
[28]HU X, BAO Y, XU Y J, et al. Final report of a prospective randomized study on thoracic radiotherapy target volume for limited-stage small cell lung cancer with radiation dosimetric analyses [J] . Cancer, 2020, 126 (4): 840-849.
[29]LINLIN G, QI W, LUNJUN Z, et al. Factors affecting the risk of brain metastasis in small cell lung cancer with surgery: Is prophylactic cranial irradiation necessary for stage Ⅰ- Ⅲdisease ?[J] Int J Radiation Oncol Biol Phys, 2013, 85 (1): 196-200.
[30]GONDI V, PUGH S, BROWN P D, et al. Significant preservation of neurocognitive func- tion (NCF) and patient-reported symptoms with hippocampal avoidance (HA) during whole brain radiotherapy for brain metastaases: final results of Ngr Oncology. CC001 [abstract] Int J Radiat Oncol Biol Phys, 2019, 105: S12-S13.
[31]XU J, YANG H, FU X, et al. Prophylactic cranial irradiation for patients with surgically resected small cell lung cancer [J] . J Thorac Oncol, 2017, 12 (2): 347-353.
[32]BROCK M V, HOOKER C M, SYPHARD J E, et al. Surgical resection of limited disease small cell lung cancer in the new era of platinum chemotherapy: Its time has come [J] . J Thorac Cardiovasc Surg, 2005, 129 (1): 64-72.
[33]YANG C F, CHAN D Y, SPEICHER P J, et al. Role of adjuvant therapy in a population-based cohort of patients with early-stage small-cell lung cancer [J] . J Clin Oncol, 2016, 34 (10): 1057-1064.





【注释】
1. 化疗
依托泊苷联合顺铂或卡铂是一线治疗的标准方案。此外,伊立替康联合铂类方案也是一线治 疗的可选择方案。由于顺铂有剂量限制性肾毒性、耳毒性、神经毒性和消化道毒性,以及治疗诱导 性耐药等缺点,对于不适用顺铂的患者,也可以选择依托泊苷联合洛铂方案。根据中国学者开展的 依托泊苷联合洛铂(EL) 对比 EP 一线治疗广泛期 SCLC 的Ⅲ期研究结果,推荐洛铂也可作为中 国广泛期 SCLC 可选的一线化疗药物。该研究共入组 234 例患者,EL 组和 EP 组中位 PFS 分别为 5.17 个月 vs 5.79 个月(P=0.182 1)、中位 OS 分别为 12.52 个月 vs 11.56 个月(P=0.338 3),DCR 为82.64% vs 83.78%(P=0.861 8)。肾毒性、恶心和呕吐的发生率在 EL 组也显著降低[7]。
2. 免疫检查点抑制剂
靶向 PD-1 和 PD-L1 的免疫检查点抑制剂在 SCLC 治疗中显示了良好的临床活性。2020 年 2 月我国国家药品监督管理局(NMPA) 基于 IMpower133 研究的结果,正式批准 PD-L1 抑制剂 atezolizumab+ 依托泊苷 / 卡铂一线治疗广泛期 SCLC 的适应证,因此本指南将其作为Ⅰ级推荐。IMpower133 研究是一项 atezolizumab+ 依托泊苷 / 卡铂对比安慰剂 + 依托泊苷 / 卡铂一线治疗广泛 期 SCLC 疗效和安全性的Ⅲ期研究[1]。结果显示,与标准治疗相比,atezolizumab 联合依托泊苷 / 卡铂可将中位 OS 延长 2 个月(12.3 个月 vs 10.3 个月,P=0.015 4),并显著提高了 12 个月(51.9% vs 30.9%)和 18 个月(34.0% vs 21.0%)的 OS 率,中位 PFS 也由 4.3 个月延长到 5.2 个月,疾病进展风险降低 23%[1,9],两组患者 3/4 级 AE 的发生率相似。在另外一种 PD-L1 抑制剂 durvalumab 联合化疗一线治疗广泛期 SCLC 的 CASPIAN 研究中,durvalumab+ 依托泊苷 / 顺铂或卡铂组的中位 OS 显著优于化疗组(13.0 个月 vs 10.3 个月,P=0.004 7),死亡风险降低 27% (HR=0.73,95%CI 0.59~0.91),两组 AE 的发生率也是相似的(98.1% vs 97%)[8]。2019 年 11 月 FDA 授予 durvalumab 在先前未接受过治疗的广泛期 SCLC 的优先审评资格,NCCN 指南也将其作为一线治疗的优先推荐。2020 年 2 月 28 日新加坡卫生科学局批准了 durvalumab 联合依托泊苷 / 卡铂或顺铂方案一线治疗广 泛期 SCLC 的适应证,但在中国尚未获批适应证,因此本指南将其作为Ⅲ级推荐。
3. 广泛期 SCLC 的胸部放疗
广泛期 SCLC 患者对一线化疗敏感者,疗效判定 CR 或 PR,且一般状态良好,加用胸部放疗可 有所获益,尤其对于胸部有残余病灶和远处转移病灶体积较小者[10]。研究证明低剂量的胸部放疗耐 受性良好,可降低症状性胸部复发风险,在一部分患者中可延长生存[11,12]。CREST 研究结果显示 全身化疗后达缓解(CR 和 PR) 的广泛期 SCLC 患者,给予胸部原发病灶放疗(30Gy/10 次) 联合 预防性脑放疗,可降低 50% 胸部复发风险,提高 2 年总体生存率(13% vs 3%,P=0.004)[13]。对 于放射治疗技术,至少应给予患者基于 CT 定位的三维适形放疗(3D-CRT),在满足足够的肿瘤剂 量并保证正常组织限量在安全范围内时,推荐使用更为先进的技术,包括(但不限于) 4D-CT 和 / 或 PET-CT 模拟定位、调强适形放疗(IMRT)/ 容积弧形调强放疗(VMAT)、图像引导放疗(IGRT) 和呼吸运动管理策略。胸部放疗的总剂量和分割次数在 30Gy/10 次到 60Gy/30 次范围内,或选择在 此范围内的等效方案。
4. PS 3~4 的广泛期 SCLC 患者
对于因 SCLC 所致的 PS 3~4 的广泛期 SCLC 患者,应充分综合考虑各种因素,谨慎选择治疗方 案,如化疗(单药方案或减量联合方案),治疗后 PS 评分能达到 2 分以上,可给予胸部放疗。如果 为非 SCLC 所致 PS 3~4 的广泛期 SCLC 患者,经对症支持治疗后,如果体力状况得到改善,PS 评 分能够达到 2 分以上,可按照 PS 0~2 组患者的治疗策略进行治疗。
5. 有局部症状的广泛期 SCLC 患者
广泛期 SCLC 转移灶姑息放疗常用于肿瘤转移到脑、脊髓、纵隔淋巴结和骨等,导致危及生命 或生活质量显著下降的患者。这些部位的放疗常常依据患者临床症状轻重缓急和化疗疗效,给予即 期或限期实施。在这些转移部位中,导致脊髓压迫症、重症上腔静脉综合征、有症状脑转移,以及 重度疼痛的骨转移,临床应考虑急诊放疗。最常用的放疗方案是 30Gy/10f/2 周。
(1)上腔静脉综合征(SVCS)患者:即期放疗的放射野原则上应包括原发灶、整个纵隔区(包 含上腔静脉区) 及两锁骨上区,但广泛期 SCLC 患者靶区勾画应遵从个体化姑息局部放疗 原则,对 PS 评分差(≥ 3) 的患者,不推荐常规采用同步放化疗[14]。此外,还需注意给 予吸氧、激素、利尿及碱化尿液、镇静、止痛等处理。
(2) 脊髓压迫症者与骨转移:这类患者通常不建议手术减压治疗,而是首先考虑局部放疗以 控制和解除压迫症状,缓解疼痛,显著改善生活质量。常用放疗方案是 30Gy/10f/2 周或 40Gy/20f/4 周;对于单个椎体转移导致脊髓压迫的患者,PS 评分差不能耐受多次放疗, 可以给予大剂量少分次放疗 20Gy/5f~8Gy/1f[15,16]。
6. 广泛期 SCLC 的头部放疗
(1) 广泛期 SCLC 在初始诊断时出现脑转移,如果没有症状,可以先以系统化疗为主,化疗 3~4 周期后择期进行头部放疗;如果有明显脑转移症状,则尽快进行头部放疗。头部放疗 建议全脑放疗(WBRT),剂量建议 30Gy/10 次。患者预期生存 4 个月以上,可以采用放 射外科(SRS) 或者立体定向放疗(SRT) 局部巩固治疗残留病灶,或者采用全脑放疗的 同时局部病灶加量的调强放疗方式(SIB-IMRT)。
(2)在 PCI 后发生脑转移,放射外科(SRS) 或者立体定向放疗(SRT) 是首选治疗[17,18], 而经过慎重选择的患者可考虑重复 WBRT[19,20]。
(3) 对于广泛期 SCLC 系统的化疗和胸部放疗后,达到很好疗效(CR/PR) 的前提下,EORTC 研究提示接受 PCI 可以提高生存率和降低后期脑转移发生概率[21],而近期日本的随机对 照研究提示,进行脑核磁检测排除颅内转移的情况下,PCI 虽然能够降低颅内转移发生的 概率(48% vs 69%,P<0.000 1),但是并不能带来生存获益[22],因此对于广泛期 SCLC 患者的 PCI 要慎重决定。
7. 老年广泛期 SCLC 的治疗
(1) 对于老年 SCLC 患者,不能仅根据年龄确定治疗方案,根据机体功能状态指导治疗更有意义。如果老年患者有日常生活自理能力、体力状况良好、器官功能相对较好,应当接受标准联合化疗(如果有指征也可放疗),但因老年患者可能有更高的概率出现骨髓抑制、乏 力和器官功能储备较差,所以在治疗过程中应谨慎观察,以避免过高的风险。
(2) 治疗方案首先考虑依托泊苷 / 铂类方案。目前尚无充分证据说明顺铂和卡铂的疗效差异, 4 个周期依托泊苷 / 顺铂的化疗方案对老年患者效果良好[23],但是考虑到顺铂可能引起严 重的肾毒性、消化道反应等不良反应,在心肺功能、肾功能不全而不适合使用顺铂的老年 患者中,5~6 周期依托泊苷联合卡铂的化疗放疗方案可能更为合理[24]。
(3)若患者无法耐受标准化疗,可进行单药方案或者减量联合方案。对体弱患者或不愿意接受 静脉用药的患者,可考虑口服依托泊苷(200mg/(m2•d)po.d1~d5,每 3~4 周重复 1 次)。对于一般情况差的患者,应以支持治疗为主。
(4)免疫检查点抑制剂治疗老年 SCLC 患者的适用性目前仍较为有 限,需进一步探 索。IMpower133 研究纳入了 186 例初治的 PS 较好的老年 SCLC 患者(大于或等于 65 岁),结 果显示 atezolizumab 联合 EC 组相比化疗组中位 OS 延长了 4.8 个月(14.4 个月 vs 9.6 个月;HR 0.59)[8]。
8. 免疫检查点抑制剂相关肺炎(checkpoint inhibitor pneumonitis,CIP)
(1)CIP 是由免疫检查点抑制剂引起的临床、影像和病理表现各异的肺损伤,处理不当可能危 及患者的生命,需引起临床医生的关注与重视。免疫检查点抑制剂单药治疗实体瘤时 CIP 的发生率 <5%,免疫联合治疗(如双免疫联合治疗、免疫联合化疗、免疫联合放疗) 可能 会增加 CIP 发生的风险[25]。
(2)在免疫检查点抑制剂联合化疗一线治疗 SCLC 的临床研究中,3~4 级肺炎的发生率为
0.5%~2%[7,8]。在一项广泛期 SCLC 的Ⅰ期研究中,33 例患者接受最多 6 周期的诱导化疗后,给予 pembrolizumab 同步放疗均未出现 CIP[26],因此目前尚无充分证据表明放疗会增加 SCLC 患者 CIP 的发生率,仍需进一步的探索[27,28]。
(3)CIP 最常见症状包括呼吸困难、咳嗽、发热、胸痛、乏力等,1/3 患者发病时可无症状。常见体征缺乏特异性,可出现呼吸频率增快、口唇发绀、肺部可闻及湿啰音等。在临床实 践中,对于接受过放疗和免疫检查点抑制剂治疗的 SCLC 患者,应注意 CIP 和放射性肺 炎的鉴别诊断,CIP 影像学表现为多磨玻璃影、斑片状实变影、小叶间隔增厚、网格影、 牵拉性支气管扩张、纤维条索影等;放射性肺炎影像学表现为多在放射野出现的斑片、实 变或纤维条索影[25]。CIP 的治疗可参考 CSCO 免疫检查点抑制剂相关的毒性管理指南。
参考文献
[1] HORN L, MANSFIELDd A S, SZCZESNA A, et al. First-line atezolizumab plus chemotherapy in extensive-stage small-cell lung cancer [J] . N Engl J Med, 2018, 379 (23): 2220-2229.
[2] SPIGEL D R, TOWNLEY P M, WATERHOUSE D M, et al. Randomized phase Ⅱ study of bevaci-zumab in combination with chemotherapy in previously untreated extensive-stage small-cell lung can- cer: results from the SALUTE trial [J] . J Clin Oncol, 2011, 29 (16): 2215-2222.
[3] OKAMOTO H, WATANABE K, NISHIWAKI Y, et al. Phase Ⅱ study of area under the plasma-concen-tration-versus-time curve-based carboplatin plus standard-dose intravenousetoposide in elderly patients with small cell lung cancer [J] . J Clin Oncol, 1999, 17 (11): 3540-3545.
[4] NODA K, NISHIWAKI Y, KAWAHARA M, et al. Irinotecan plus cisplatin compared with etoposide plus cisplatin for extensive small-cell lung cancer [J] . N Engl J Med, 2002, 346 (2): 85-91.
[5] HANNA N, BUNN J R. P A, LANGER C, et al. Randomized phase Ⅲtrial comparing irinotecan/cis- platin with etoposide/cisplatin in patients with previously untreated extensive-stage disease small-cell lung cancer [J] . J Clin Oncol, 2006, 24 (13): 2038-2043.
[6] SCHMITTEL A, FISCHER V L, SEBASTIAN M, et al. A randomized phase Ⅱtrial of irinotecan plus carboplatin versus etoposide plus carboplatin treatment in patients with extended disease small cell lung cancer [J] . Ann Oncol, 2006, 17 (4): 663-667.
[7] CHENG Y, FAN Y, LIU X, et al. Randomized controlled trial of lobaplatin plus etoposide vs. cisplatin plus etoposide as first-line therapy in patients with extensive-stage small cell lung cancer [J] . Oncol Lett, 2019, 17 (5): 4701-4709.
[8] PAZ-ARES L, DVORKIN M, CHEN Y, et al. Durvalumab plus platinum-etoposide versus plati- num-etoposide in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): a ran- domised, controlled, open-label, phase 3 trial [J] . Lancet, 2019, 394 (10212): 1929-1939.
[9] MARTIN R, STEPHEN V, AARON S, et al. IMPOWER133: updated overall survival (OS) analy-sis of first line (1L) atezolizumab (atezo) + carboplatin + etoposide in extensive stage sclc (ES-SCLC) [J] . ESMO, 2019, 17360.
[10] JEREMIC B, CASAS F, WANG L, et al. Radiochemotherapy in extensive disease small cell lung cancer ED-SCLC [J] . Front Radia Ther Oncol, 2010, 42: 180-186.
[11] JEREMIC B, SHIBAMOTO Y, NIKOLIC N, et al. Role of radiation therapy in the combined-modal-ity treatment of patients with extensive disease small-cell lung cancer: A randomized study [J] . J Clin Oncol, 1999, 17 (7): 2092-2099.
[12] YEE D, BUTTS C, REIMAN A, et al. Clinical trail of post-chemotherapy consolidation thoracic radiotherapy for extensive-stage small cell lung cancer [J] . Radiother Oncol, 2012, 102 (2): 234-238.
[13] SLOTMAN B J, VAN TINTEREN H, PRAAG J Q, et al. Use of thoracic radiotherapy for extensive stage small cell lung cancer: a phase 3 randomised controlled trail [J] . Lan- cet, 2015, 385 (9962): 36-42.
[14] CHAN R H, DAR A R, YU E et al. Superior vena cava obstruction in small-cell lung cancer [J] . Int J Radiat Oncol Biol Phys, 1997, 38 (3): 513-520.
[15] CHOW E, HOSKIN P, MITERA G, et al. Update of the international consensus on palliative radiotherapy endpoints for future clinical trials in bone metastases [J] . Int J Radiat Oncol Biol Phys, 2012, 82 (5): 1730-1737.
[16] HOSKIN P, HOWELL D, KONSKI A, et al. Palliative Radiotherapy for Bone Metastases: an ASTRO evidence-based guideline [J] . Int. J. Radiation Oncology Biol. Phys, 2011, 79 (4): 965-976.
[17] HARRIS S, CHAN M D, LOVATO J F, et al. Gamma knife stereotactic radiosurgery as salvage ther- apy after failure of whole-brain radiotherapy in patients with small-cell lung cancer [J] . Int J Radiat Oncol Biol Phys, 2012, 83 (1): e53-e59.
[18] WEGNER R E, OLSON A C, KONDZIOLKA D, et al. Stereotactic radiosurgery for patients with brain metastases from small cell lung cancer [J] . Int J Radiat Oncol Biol Phys, 2011, 81 (3): e21-e27.
[19] SADIKOV E, BEZJAK A, YI Q L, et al. Value of whole brain re-irradiation for brain metastases— single centre experience [J] . Clin Oncol (R Coll Radiol. ) , 2007, 19 (7): 532-538.
[20] SON CH, JIMENEZ R, NIEMIERKO A, et al. Outcomes after whole brain reirradiation in patients with brain metastases [J] . Int J Radiat Oncol Biol Phys, 2012, 82 (2): e167-e172.
[21] SLOTMAN B, FAIVRE-FINN C, KRAMER G, et al. Prophylactic cranial irradiation in extensive small-cell lung cancer [J] . N Engl J Med, 2007, 357 (7): 664-672.
[22] TAKAHASHI T, YAMANAKA T, SETO T, et al. Prophylactic cranial irradiation versus observa-tion in patients with extensive-disease small-cell lung cancer: a multicentre, randomised, open- label, phase 3 trial [J] . Lancet Oncol, 2017, 18 (5): 663-671.
[23] OKAMOTO H, WATANABE K, NISHIWAKI Y, et al. Phase Ⅱstudy of area under the plasma-con-centration-versus-time curve-based carboplatin plus standard-dose intravenous etoposide in elderly patients with small-cell lung cancer [J] . J Clin Oncol, 1999, 17 (11): 3540-3545.
[24] MATSUI K, MASUDA N, YANA T, et al. Carboplatin calculated with Chatelut’s formula plus etopo-side for elderly patients with small-cell lung cancer [J] . Intern Med, 2001, 40 (7): 603-606.
[25] 中华医学会呼吸病学分会肺癌学组 . 免疫检查点抑制剂相关肺炎诊治专家共识 [J] . 中华结核 和呼吸杂志 , 2019, 42 (11): 820-825.
[26] WELSH J W, HEYMACH J V, CHEN D, et al. Phase I trial of pembrolizumab and radiation therapy after induction chemotherapy for extensive-stage small cell lung cancer [J] . J Thorac Oncol, 2019, pii: S1556-0864 (19) : 33525-33527.
[27] NESBIT E G, LEAL T A, KRUSER T J. What is the role of radiotherapy for extensive-stage small cell lung cancer in the immunotherapy era ?[J] Transl Lung Cancer Res, 2019, 8 (Suppl 2): S153-S162.
[28] VERMA V, CUSHMAN T R, SELEK U, et al. Safety of Combined Immunotherapy and Thoracic Radiation Therapy: Analysis of 3 Single-Institutional Phase Ⅰ/ ⅡTrials [J] . Int J Radiat Oncol Biol Phys, 2018, 101 (5): 1141-1148.






【注释】
1. 尽管 SCLC 对于初始治疗非常敏感,但大多数的 SCLC 患者在初始治疗后出现复发及耐药;这些患者在接受进一步的化疗后中位 OS 只有 4~5 个月[17,18]。尽管治疗的有效率很大程度上取 决于初始治疗结束至复发的时间间隔,但在多数患者二线治疗也能显著缓解症状。
2. 距离一线治疗结束≤ 6 个月内复发或进展者,推荐二线治疗选择拓扑替康、伊立替康、吉西他 滨、紫杉醇或长春瑞滨等药物治疗,同时也推荐进入临床试验。拓扑替康有静脉和口服两种给 药方式,一项Ⅲ期研究证实口服拓扑替康的疗效及耐受性与静脉给药相似,ORR 分别 18.3% 和 21.9%,OS 分别为 33 周和 35 周,口服用药更方便[3]。粒细胞减少是拓扑替康主要的剂量 限制性毒性,有研究证实拓扑替康 1.25mg/m2 与 1.5mg/m2 静脉给药的疗效相当,且 3~4 级血液 学毒性明显降低[19]。在中国,静脉给药拓扑替康获批的用药剂量为 1.25mg/m2,连续 5 天,每 21 天为一周期,并在多个Ⅱ期研究中证实了在中国人群中的疗效和安全性[20,21]。
3. 距离一线治疗结束 >6 个月复发或进展者,可选择初始治疗方案。但对于既往 atezolizumab 或 durvalumab 维持治疗 >6 个月后复发的患者,不推荐重新使用 PD-L1 抑制剂 + 化疗的联合方案, 建议可使用卡铂 + 依托泊苷或顺铂 + 依托泊苷方案。
4. 后续治疗最佳的周期数仍无定论,由于细胞毒药物的毒性,建议在患者接受化疗取得最佳疗效后再用药 2 个周期。
参考文献
[1] VON PAWEL J, SCHILLER J H, SHEPHERD F A, et al. Topotecan versus cyclophospha-mide, doxorubicin, and vincristine for the treatment of recurrent small-cell lung cancer [J] . J Clin Oncol, 1999, 17(2): 658-667.
[2] O BRIEN M E, CIULEANU T E, TSEKOV H, et al. Phase Ⅲ trial comparing supportive care alone with supportive care with oral topotecan in patients with relapsed small-cell lung cancer [J] . J Clin Oncol, 2006, 24(34): 5441-5447.
[3] ECKARDT J R, VON PAWEL J, PUJOL J L, et al. Phase Ⅲstudy of oral compared with intravenous topotecan as second-line therapy in small-cell lung cancer [J] . J Clin Oncol, 2007, 25(15): 2086-2092.
[4] MASUDA N, FUKUOKA M, KUSUNOKI Y, et al. CPT-11: a new derivative of camptothecin for the treatment of refractory or relapsed small-cell lung cancer [J] . J Clin Oncol, 1992, 10(8): 1225-1229.
[5] SMIT E F, FOKKEMA E, BIESMA B, et al. A phaseⅡstudy of paclitaxel in heavily pretreated patients with small-cell lung cancer [J] . Br J Cancer, 1998, 77(2): 347-351.
[6] YAMAMOTO N, TSURUTANI J, YOSHIMURA N, et al. PhaseⅡstudy of weekly paclitaxel for relapsed and refractory small cell lung cancer [J] . Anticancer Res, 2006, 26(1B): 777-781.
[7] SMYTH J F, SMITH I E, SESSA C, et al. Activity of docetaxel (Taxotere) in small cell lung can-cer. The Early Clinical Trials Group of the EORTC [J] . Eur J Cancer, 1994, 30A(8): 1058-1060.
[8] VAN DER LEE I, SMIT E F, VAN PUTTEN J W, et al. Single-agent gemcitabine in patients with resistant small-cell lung cancer [J] . Ann Oncol, 2001, 12(4): 557-561.
[9] MASTERS G A, DECLERCK L, BLANKE C, et al. Phase Ⅱtrial of gemcitabine in refractory or relapsed small cell lung cancer: Eastern Cooperative Oncology Group Trial 1597 [J] . J Clin Oncol, 2003, 21(8): 1550-1555.
[10] EINHORN L H, PENNINGTON K, MCCLEAN J. PhaseⅡ trial of daily oral VP-16 in refractory small cell lung cancer: a Hoosier Oncology Group study [J] . Semin Oncol, 1990, 17(1 Suppl 2): 32-35.
[11] JOHNSON D H, GRECO F A, STRUPP J, et al. Prolonged administration of oral etopo- side in patients with relapsed or refractory small-cell lung cancer: a phase Ⅱ trial [J] . J Clin Oncol, 1990, 8(10): 1613-1617.
[12] JASSEM J, KARNICKA-MLODKOWSKA H, VAN POTTELSBERGHE C, et al. Phase Ⅱstudy of vinorelbine (Navelbine) in previously treated small cell lung cancer patients. EORTC Lung Cancer Cooperative Group [J] . Eur J Cancer, 1993, 29A(12): 1720-1722.
[13] FURUSE K, KUBOA K, KAWAHARA M, et al. PhaseⅡstudy of vinorelbine in heavily previ-ously treated small cell lung cancer. Japan Lung Cancer Vinorelbine Study Group [J] . Oncol- ogy, 1996, 53(2): 169-172.
[14] PIETANZA M C, KADOTA K, HUBERMAN K, et al. Phase Ⅱtrial of temozolomide with relapsed sensitive or refractory small cell lung cancer, with assessment of methylguanine-DNA methyltrans- ferase as a potential biomarker [J] . Clin Cancer Res, 2012, 18(4): 1138-1145.
[15] ZAUDERER M G, DRILON A, KADOTA K, et al. Trial of a 5-day dosing regimen of temozolomide in patients with relapsed small cell lung cancers with assessment of methylguanine-DNA methyl-transferase [J] . Lung Cancer, 2014, 86(2): 237-240.
[16] LAMMERS P E, SHYR Y, LI C I, et al. PhaseⅡstudy of bendamustine in relapsed chemotherapy sensitive or resistant small-cell lung cancer [J] . J Thorac Oncol, 2014, 9(4): 559-562.
[17] HURWITZ J L, MCCOY F, SCULLIN P, et al. New advances in the second-line treatment of small cell lung cancer [J] . Oncologist, 2009, 14(10): 986-994.
[18] SCHNEIDER B J. Management of recurrent small cell lung cancer [J] . J Natl Compr Canc Netw, 2008, 6(3): 323-331.
[19] HUBER R M, RECK M, GOSSE H, et al. Efficacy of a toxicity-adjusted topotecan therapy in recur-rent small cell lung cancer [J] . Eur Respir J, 2006, 27(6): 1183-1189.
[20] 张力 , 夏忠军 , 管忠震 , 等 . 拓扑替康治疗小细胞肺癌Ⅱ期临床研究 [J] . 癌症 , 2001, 20(4): 419- 422.
[21] 程文元 , 王华庆 . 国产盐酸拓扑替康治疗小细胞肺癌Ⅱ期临床研究 [J] . 中国肿瘤 , 2001,10(8): 495-496.

【注释】
1. 二线治疗失败的 SCLC 患者,如果 PS 评分为 0~2 分,可以考虑后续的三线及以上治疗。
2. 安罗替尼
安罗替尼是我国自主研发的一种新型小分子多靶点酪氨酸激酶抑制剂,能有效抑制 VEGFR、 PDGFR、FGFR、c-Kit 等激酶,具有抗肿瘤血管生成和抑制肿瘤生长的作用。我国研究者开展的安 罗替尼对比安慰剂三线及以上治疗 SCLC 的Ⅱ期研究(ALTER1202) 结果显示,安罗替尼将 SCLC 患者的 PFS 延长了 3.4 个月(4.1 个月 vs 0.7 个月),疾病进展风险降低了 81%[1]。OS 亦有显著获益, 安罗替尼组为 7.3 个月,安慰剂组为 4.9 个月,HR 0.53[2]。亚组分析中,脑转移患者的 PFS 延长了 3 个月(3.8 个月 vs 0.8 个月,HR 0.15),OS 延长了 3.7 个月(6.3 个月 vs 2.6 个月,HR 0.23)[5]。安罗 替尼的安全性易于管理,并且具有口服用药的便利优势,更容易被患者接受。2019 年 9 月 NMPA批准了安罗替尼三线及以上治疗 SCLC 的适应证,因此本指南推荐安罗替尼作为 SCLC 三线及以上 治疗的Ⅰ级推荐。
3.nivolumab
Ⅰ/ Ⅱ期 CheckMate032 研究证实复治 SCLC 患者接受 nivolumab 3mg/kg 单药治疗的患 者 ORR 为 10%,接受 nivolumab 1 mg/kg+ipilimumab 3mg/kg 治疗患者的 ORR 为 23%,接受 nivolumab 3mg/kg+ipilimumab 1mg/kg 治疗患者的 ORR 为19%[6]。在 TMB 人群的探索性分析中, nivolumab+ipilimumab 治疗高 TMB 患者的有效率可达 46.2%,1 年 PFS 率为 30.0%,显著优于低、 中 TMB 亚组[7];在该研究 nivolumab 单药三线治疗的亚组分析中,ORR 为 11.9%,中位缓解持 续时间(DoR)为 17.9 个 月,中位 PFS 为 1.4 个月(95%CI 1.3~1.6),6 个月 PFS 17.2%(95%CI 10.7~25.1),中位 OS 为 5.6 个月(95%CI 3.1~6.8),12 个月 OS 为 28.3%(95%CI 20.0~37.2),18 个月 OS 为 20.0%(95%CI 12.7~28.6)[3],基于此结果,FDA 批准 nivolumab 单药用于治疗既往接受 过含铂方案化疗以及至少一种其他疗法后疾病进展的转移性 SCLC 患者。由于 nivolumab 在中国未 获批 SCLC 适应证,故本指南Ⅱ级推荐其作为复发 SCLC 的三线及以上治疗。
4.pembrolizumab
KEYNOTE028/158 研究汇总分析结果显示,pembrolizumab 三线及以上治疗 SCLC 的 ORR 为 19.3%(95%CI 11.4~29.4)。DoR 未达到(范围 4.1~35.8 个月),超过 12 个月的 DoR 率为 67.7%,超 过 18 个月 DoR 率为 60.9%。PFS 为 2.0 个月(95%CI 1.9~3.4),12 个月和 24 个月的 PFS 率分别为 16.9% 和 13.1%。中位 OS 为 7.7 个月(95%CI 5.2~10.1),12 个月和 24 个月 OS 率分别为 34.2% 和20.7%[4]。基于此结果,FDA 批准 pembrolizumab 单药用于治疗既往接受过含铂方案化疗以及至少 一种其他疗法后疾病进展的转移性 SCLC 患者。由于 pembrolizumab 在中国未获批 SCLC 适应证, 故本指南将其作为Ⅱ级推荐用于复发 SCLC 的三线及以上治疗。
参考文献
[1] CHENG Y, WANG Q M, LI K, et al. Anlotinib as third-line or further-line treatment in relapsed SCLC: a multicentre, randomized, double-blind phase 2 trial. 2018 World Conference on Lung Can- cer. Abstract. OA13. 03.
[2] CHENG Y, WANG Q M, Li K, et al. Overall survival (OS) update in ALTER 1202: Anlotinib as third-line or further-line treatment in relapsed SCLC. European Society for Medical Oncology Congress 2019. Abstract. 17380.
[3] READY N, FARAGO A F, Braud F, et al. Third-line nivolumab monotherapy in recurrent SCLC: CheckMate 03 [J] . J Thorac Oncol, 2019, 14 (2) : 237-244.
[4] CHUNG H C, PIHA-PAUL S A, LOPEZ-MARTIN J, et al. Pembrolizumab after two or more lines of previous therapy in patients with recurrent or metastatic SCLC: results from the KEYNOTE-028 and KEYNOTE-158 studies [J] . J Thorac Oncol, 2019, pii: S1556-0864 (19): 33850-X.
[5] CHENG Y, WANG Q M, LI K, et al. The impact of Anlotinib for relapsed SCLC patients with brain metastases: a subgroup analysis of ALTER 1202. 2019 World Conference on Lung Can- cer. Abstract. P2. 12-26.
[6] ANTONIA SJ, LOPEZ-MARTIN J A, Bendell J, et al. Nivolumab alone and nivolumab plus ipilimumab in recurrent small-cell lung cancer (CheckMate 032) : a multicentre, open-label, phase 1/2 trial [J] . Lancet Oncol, 2016, 17 (7) : 883-895.
[7] RIZVI N, ANTONIA S, CALLAHAN M K, et al. Impact of tumor mutation burden on the efficacy of nivolumab or nivolumab plus ipilimumab in small cell lung cancer: An exploratory analysis of Check- Mate 032. 2017 World Conference on Lung Cancer. Abstract OA 07. 03a.










参考文献
[1]王绿化 , 傅小龙 , 陈明 , 等 . 放射性肺损伤的诊断及治疗 [J] . 中华放射肿瘤学杂志 , 2015, 24(1): 4-9.
[2]LALLA R V, BOWEN J, BARASCH A, et al. MASCC/ISOO clinical practice guidelines for the man-agement of mucositis secondary to cancer therapy [J] . Cancer, 2014, 120(10): 1453-1461.
[3]MOVSAS B, SCOTT C, LANGER C, et al. Randomized trial of amifostine in locally advanced non- small-cell lung cancer patients receiving chemotherapy and hyperfractionated radiation: radiation therapy oncology group trial 98-01 [J] . J Clin Oncol, 2005, 23(10): 2145-2154.
[4] 于金明 , 井 旺 , 朱 慧 , 等 . 急性放射性黏膜炎治疗现状 [J] . 中华放射医学与防护杂志 ,2015, 35(3): 233-235.
[5] LALLA R V, BOWEN J, BARASCH A, et al. MASCC/ISOO clinical practice guidelines for the man- agement of mucositis secondary to cancer therapy [J] . Cancer, 2014, 120(10): 1453-1461.
[6] RYU S H, KANG K M, MOON S Y, et al. Therapeutic effects of recombinant human epidermal growth factor (rhEGF) in a murine model of concurrent chemo-and radiotherapy-induced oral mucosi- tis [J] . J Radiat Res, 2010, 51(5): 595-601.

【注释】
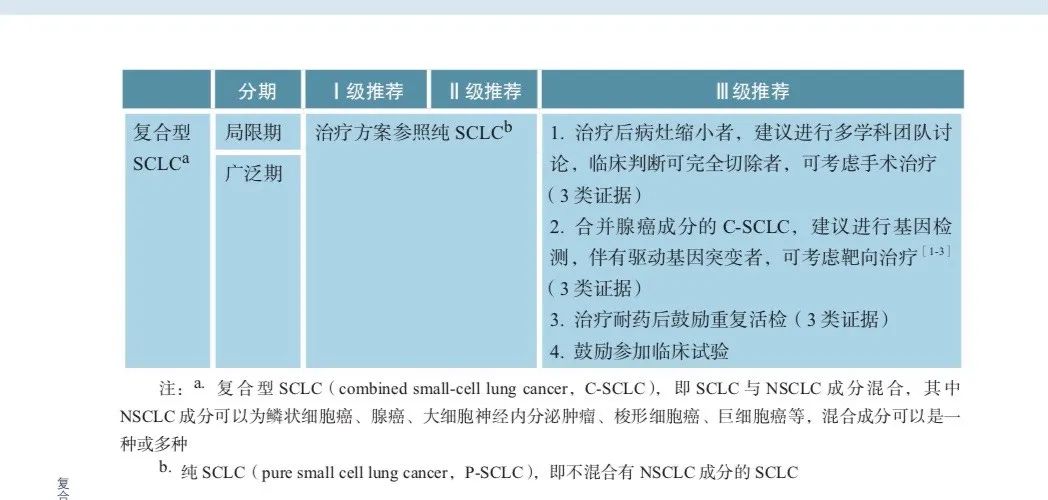
复合型小细胞肺癌(C-SCLC) 的治疗至今尚缺乏大样本前瞻性随机对照临床研究数据,绝大多数为小样本回顾性分析和个案报道。因此目前各大指南均将 C-SCLC 归为 SCLC 范畴,采用同样的治疗模式,缺乏更为个体化和具体的治疗策略。
1. 手术治疗
如系统分期检查后无纵隔淋巴结转移的 T1-2N0 局限期患者可考虑手术切除,手术方式首选肺 叶切除术 + 肺门、纵隔淋巴结清扫术。一项小样本回顾性分析显示,Ⅰ期 C-SCLC 患者术后 5 年生存率为 31%。另一项回顾性分析显示 LD 期 C-SCLC 患者接受手术切除者的 5 年生存率显著高于未 手术者(48.9%vs 36.6%)。手术不仅有助于 C-SCLC 的诊断,并且与纯小细胞肺癌(P-SCLC) 相比 C-SCLC 接受手术切除的获益更显著[4]。术后进行依托泊苷 + 顺铂(EP) 或依托泊苷 + 卡铂(EC) 方案辅助化疗能够提高 C-SCLC 患者的预后。对于术后 N1-2 的患者推荐进行术后辅助放疗,预防性脑放疗作为可选策略。
2. 化疗和放疗
对于超过 T1-2N0 且 PS 评分 0~2 分的局限期患者,基本治疗策略为化疗联合放疗(同步或序贯), 化疗方案可选择 EP 或 EC 方案。疗效达到 CR 或 PR 者可考虑行预防性 PCI[5]。PS 评分为 3~4 分的局限期患者基本策略为化疗或最佳支持治疗,放疗和PCI作为可选策略。广泛期患者的基本治疗策略 为 EP/EC 或伊立替康联合顺铂 / 卡铂(IP/IC) 的化疗方案。对于达到 CR 或 PR 的患者可行胸部放 疗和预防性 PCI[6-9]。
C-SCLC 化疗敏感性较 P-SCLC 低,有效率在 50% 左右,可能与混杂了 NSCLC 细胞成分有关[10]。然而,C-SCLC 的优选化疗方案尚未明确,需要将 SCLC 和 NSCLC 均纳入考虑的个体化治疗方 案。一项回顾性研究比较了长春瑞滨 + 异环磷酰胺 + 顺铂(NIP) 三药联合方案与 EP 方案在167 例Ⅲ~ Ⅳ期 C-SCLC 一线治疗中的疗效,结果显示 NIP 组和 EP 组的 ORR 分别为 30.0% 和38.5%,中位 PFS 分别为 6.0 个月和 6.5 个月,MST 分别为 10.4 个月和 10.8 个月,均无统计学差异;并且 NIP 组不良反应发生率和程度更高。另一项回顾性研究在 62 例 C-SCLC 中比较了紫杉醇 + 依托 泊苷 + 顺铂 / 卡铂(TEP/TCE) 三药联合方案与 EP/EC 方案一线治疗的疗效,TEP/TCE 组的 ORR 高于 EP/CE 组,具有统计学差异(90%vs 53%,P=0.033),而 DCR 无统计学差异(100%vs 86%, P = 0.212) ;TEP/TCE 组在中位 PFS 和 MST 方面均略有延长,但未达到统计学差异(10.5 个月 vs 8.9 个 月,P = 0.484 ;24.0 个月 vs 17.5 个月,P = 0.457)。三药联合组不良反应发生率和程度更高。以上 研究表明,三药联合方案的疗效并未优于两药方案且耐受性更差,仍不能取代 EP/EC 标准方案。
目前评估放疗在 C-SCLC 中作用的研究尚未见报道。但多数观点认为,C-SCLC 对于放疗的敏 感性可能同样低于纯 SCLC,放疗能否改善 C-SCLC 患者的 OS 仍有待于更深入的研究。
3. 靶向和免疫治疗
驱动基因突变在 SCLC 中非常少见,据报道 EGFR 突变在纯 SCLC 中发生率约 4%,而在 C-SCLC 可达到 15%~20%,多发生在无或有轻度吸烟史且混合腺癌成分的 C-SCLC[11-13]。由于临床上并未对 SCLC 进行常规基因检测,实际突变率可能更高。目前已经报道多例携带 EGFR 突变的 SCLC 和混 杂腺癌成分的 C-SCLC 接受 EGFR 酪氨酸激酶抑制剂治疗有效的个案[14-16]。这提示靶向治疗可能在 混杂腺癌成分且合并驱动基因突变 C-SCLC 的治疗中具有潜在获益对于合并腺癌成分 C-SCLC 进行 基因检测和重复活检或许可作为实现 C-SCLC 个体化治疗的策略。
SCLC 多存在基因组和染色体高度不稳定性,造成突变频率增加,理论上可能对免疫治疗更敏感。据报道 C-SCLC 中同样存在 TP53、RB1、PTEN 等大量高频突变。免疫治疗已在 SCLC 一线及 三线治疗中取得突破,然而免疫治疗对于 C-SCLC 仍是未来需要深入探索的全新领域。
综上所述,C-SCLC 作为 SCLC 的特殊类型,其来源、生物学特性等问题仍不十分清楚,以往 研究多以回顾性分析和病例报道为主,缺乏大样本前瞻性研究数据为支持的高级别循证医学证据。因此,对于 C-SCLC 的治疗还有很多争议和未知,尚未达成全面和广泛的临床指南和专家共识,有 待于未来更为深入的研究来进行修正和补充。
参考文献
[1] OKAMOTO I, ARAKI J, SUTO R, et al. EGFR mutation in gefitinib-responsive small-cell lung can- cer [J] . Ann Oncol, 2006, 17(6): 1028-1029.
[2] ZAKOWSKI M F, LADANYI M, KRIS M G. EGFR mutations in small-cell lung cancers in patients who have never smoked [J] . N Engl J Med, 2006, 355(2): 213-215.
[3] TAKAGI Y, NAKAHARA Y, HOSOMI Y, et al. Small-cell lung cancer with a rare epidermal growth factor receptor gene mutation showing“wax-and wane”transformation [J] . BMC Can- cer, 2013, 13: 529.
[4] BABAKOOHI S, FU P, YANG M, et al. Combined SCLC clinical and pathologic characteris- tics [J] . Clin Lung Cancer, 2013, 14(2): 113-119.
[5] AUPERIN A, ARRIAGADA R, PIGNON J P, et al. Prophylactic cranial irradiation for patients with small-cell lung cancer in complete remission. Prophylactic Cranial Irradiation Overview Collaborative Group [J] . N Engl J Med, 1999, 341(7): 476-484.
[6] JEREMIC B, SHIBAMOTO Y, NIKOLIC N, et al. Role of radiation therapy in the combined-modality treatment of patients with extensive disease small-cell lung cancer: A randomized study [J] . J Clin Oncol, 1999, 17(7): 2092-2099.
[7] YEE D, BUTTS C, REIMAN A, et al. Clinical trial of post-chemotherapy consolidation thoracic radio-therapy for extensive-stage small cell lung cancer [J] . Radiother Oncol, 2012, 102(2): 234-238.
[8] SLOTMAN BJ, VAN TINTEREN H, PRAAG JO, et al. Use of thoracic radiotherapy for extensive stage small-cell lung cancer: a phase 3 randomised controlled trial [J] . Lancet, 2015, 385(9962): 36-42.
[9] SLOTMAN B, FAIVRE-FINN C, KRAMER G, et al. Prophylactic cranial irradiation in extensive small-cell lung cancer [J] . N Engl J Med, 2007, 357(7): 664-672.
[10] RADICE PA, MATTHEWS MJ, IHDE DC, et al. The clinical behavior of“mixed”small cell/large cell bronchogenic carcinoma compared to“pure”small cell subtypes [J] . Can- cer, 1982, 50(12): 2894-2902.
[11] TATEMATSU A, SHIMIZU J, MURAKAMI Y, et al. Epidermal growth factor receptor mutations in small cell lung cancer [J] . Clin Cancer Res, 2008, 14(19): 6092-6096.
[12] LU HY, MAO WM, CHENG QY, et al. Mutation status of epidermal growth factor receptor and clinical features of patients with combined small cell lung cancer who received surgical treat- ment [J] . Oncol Lett, 2012, 3(6): 1288-1292.
[13] LU HY, SUN WY, CHEN B, et al. Epidermal growth factor receptor mutations in small cell lung cancer patients who received surgical resection in China [J] . Neoplasma, 2012, 59(1): 100-104.
[14] HAGE R, ELBERS J R, BRUTEL D L R A, et al. Surgery for combined type small cell lung carci- noma [J] . Thorax, 1998, 53(6): 450-453.
[15] MEN Y, HUI Z, LIANG J, et al. Further understanding of an uncommon disease of combined small cell lung cancer: clinical features and prognostic factors of 114 cases [J] . Chin J Cancer Res, 2016, 28(5): 486-494.
[16] BABAKOOHI S, FU P, YANG M, et al. Combined SCLC clinical and pathologic characteris-tics [J] . Clin Lung Cancer, 2013, 14(2): 113-119.


【注释】
1. 副瘤综合征的分类
SCLC 是最常见的伴发副瘤综合征的组织学类型,根据发病机制可分为内分泌性副瘤综合征和 神经系统副瘤综合征。内分泌性副瘤综合征的发病机制为肿瘤细胞异位激素分泌引起神经内分泌系统的临床症状;神经系统副瘤综合征的发病机制为肿瘤细胞表达神经系统抗原从而与神经组织产生交叉免疫反应,导致神经系统功能障碍[1]。
2. 内分泌性副瘤综合征
SCLC 可以异位分泌多种激素或具有内分泌功能的多肽物质,除了分泌抗利尿激素(ADH)、促肾上腺皮质激素(ACTH) 外,还包括催乳素、生长激素、肾素等激素,可出现溢乳、闭经、高血压等临床表现。
3.抗利尿激素异常分泌综合征(syndrome of inappropriate ADH secretion,SIADH)
SIADH 的诊断标准尚不统一,有研究将其定为尿液渗透压阈值低于 100mOsm/L[2],也有研究 将血清钠浓度低于 135mmol/L 定义抗利尿激素异常分泌综合征[3]。目前,尚未开展治疗 SIADH 的 前瞻性、随机临床研究,但对于轻、中度低钠血症患者的治疗也应得到重视。治疗策略包括静脉应 用高渗盐水及口服去甲环素、碳酸锂等药物;重度、难治的低钠血症可以考虑使用加压素受体拮抗 剂治疗,推荐的药物包括考尼伐坦和托伐普坦等[4,5]。
4.库欣(Cushing) 综合征
除全身化疗外,可使用酮康唑、美替拉酮、依托咪酯、米托坦和米非司酮减少糖皮质激素生成[6-8]。自 1985 年首次报道以来,酮康唑被广泛用于外源性库欣(Cushing) 综合征的治疗,但是因为它是 细胞色素 P450 3A4 的强抑制剂,需警惕酮康唑增加化疗毒性的风险,因此美替拉酮被认为是更好 的选择[9]。对于重度促肾上腺皮质激素依赖性库欣(Cushing)综合征患者,为早期控制皮质醇水平, 美替拉酮与酮康唑联合或米托坦、美替拉酮、酮康唑联合治疗可作为替代方案。
5.兰伯特 - 伊顿(Lambert-Eaton) 综合征
本病又称肿瘤肌无力综合征,是一种由免疫介导的神经 - 肌肉接头功能障碍性疾病,是 SCLC最常伴发的神经系统副瘤综合征,1%~3% 的 SCLC 患者初诊时以该病就诊[1]。
6. 抗 Hu 抗体介导的综合征
该副瘤综合征的特征表现是炎症反应和神经元缺失,SCLC 肿瘤细胞特异性抗原导致机体抗 Hu 抗体的产生,抗 Hu 抗体作用于神经元 RNA 结合蛋白而引起临床症状。导致每种副瘤综合征不同临 床表现的原因尚不明确,并不是所有确诊病例都能检测到抗 Hu 抗体[1]。
参考文献
[1] 程颖 , 孙燕 , 吴一龙 . 小细胞肺癌[M]. 北京 : 人民卫生出版社 , 2014.
[2] GROHE C, BERARDI R, BURST V. Hyponatraemia—SIADH in lung cancer diagnostic and treat- ment algorithms [J] . Critical Reviews in Oncology, 2015, 96(1): 1-8.
[3] HOORN E J, TUUT M K, HOORNTJE S J, et al. Dutch guideline for the management of electrolyte disorders-2012 revision [J] . Netherlands Journal of Medicine, 2013, 71(3): 153-165.
[4] TRUMP D L. Serious hyponatremia in patients with cancer: Management with demeclocy- cline [J] . Cancer, 1981, 47(12): 2908-2912.
[5] JACOT W, COLINET B, BERTRAND D, et al. Quality of life and comorbidity score as prognostic determinants in non-small-cell lung cancer patients [J] . Annals of Oncology, 2008, 19(8): 1458-1464.
[6] ATKINSON A B. The treatment of Cushing’s disease [J] . Clinical Endocrinology, 1991, 34(6): 507- 513.
[7] PILLANS P I, COWAN P, WHITELAW D. Hyponatraemia and confusion in a patient taking ketocon-azole [J] . Lancet, 1985, 325(8432): 821-822.
[8] SCHILLER J H, JONES J C. Paraneoplastic syndromes associated with lung cancer [J] . Current Opin- ion in Oncology, 1993, 5(2): 335-342.
[9] SHEPHERD F A, HOFFERT B, EVANS W K, et al. Ketoconazole. Use in the treatment of ecto-pic adrenocorticotropic hormone production and Cushing’s syndrome in small-cell lung can- cer [J] . Archives of Internal Medicine, 1985, 145(5): 863-864.









【注释】
1. 肿瘤负荷低、无症状、低级别患者
可暂予观察,每 3~6 个月复查胸部增强 CT 和腹部 / 盆腔多时相 CT/MRI。也有部分患者可开始 奥曲肽或兰瑞肽治疗。对于这类患者使用奥曲肽或兰瑞肽治疗的时机尚无明确的共识,尽管在这些 患者中可以考虑开始使用奥曲肽或兰瑞肽,但直至肿瘤进展时再开始使用奥曲肽或兰瑞肽也可能适 用于部分患者。
2. 伴有明显肿瘤负荷、低级别肺或胸腺肿瘤患者
可考虑开始使用奥曲肽和兰瑞肽。治疗晚期低度恶性肿瘤的其他方法,包括使用依维莫司或替 莫唑胺。两种治疗方法都可以联合或不联合奥曲肽。
3. 晚期中级别肺或胸腺神经内分泌肿瘤患者
一般应首选全身治疗,包括开始使用奥曲肽和兰瑞肽治疗。其他选择包括依维莫司,替莫唑胺[6], 卡铂或顺铂联合依托泊苷治疗。顺铂 / 依托泊苷、卡铂 / 依托泊苷或替莫唑胺可考虑用于 Ki-67、核 分裂指数和分级方面不典型级别较高的肿瘤,尤其是组织学上分化较差的肿瘤[4]。这些治疗可联合 或不联合奥曲肽或兰瑞肽。对于肿瘤增殖指数较低的患者,亦可推荐观察。如果在一线治疗中发现 疾病进展,建议更改后续治疗方案。
4. 多发性先天性肺神经内分泌细胞增生
发病罕见,但仍有少部分患者表现为肺部多发结节和沿外周气道播散的神经内分泌细胞增生, 这种情况下可诊断为多发性先天性肺神经内分泌细胞增生(DIPNECH)。该病通常呈惰性,建议患者观察,每 12~24 个月或出现新的症状时复查胸部平扫 CT。
5. 化疗
晚期神经内分泌肿瘤对化疗反应率普遍较低,没有明确的 PFS 获益[7]。一项Ⅱ期研究评估了卡 培他滨治疗转移性类癌的疗效,19 例患者有 13 例达到疾病控制,未出现肿瘤缓解的患者[8]。另一 项Ⅱ期研究评估了卡培他滨联合奥沙利铂的疗效,在低分化神经内分泌肿瘤患者中有效率为 23%, 高分化患者有效率为 30%[9]。晚期类癌患者对替莫唑胺的应答率很低[10]。对于有临床症状的支气 管肺或胸腺低 / 中级别神经内分泌肿瘤患者,可以使用替莫唑胺单药、替莫唑胺与奥曲肽或兰瑞肽 联合使用来控制肿瘤负荷或相关症状[5,11]。一项 31 例进展期转移性支气管神经内分泌肿瘤的回顾 性研究显示,替莫唑胺单药有效率为 14%[11]。
6. 依维莫司
对于晚期中级别(不典型类癌) 支气管肺神经内分泌肿瘤,依维莫司是可选的一种治疗策略。在一项Ⅱ期研究中,使用依维莫司与长效奥曲肽联合治疗晚期神经内分泌肿瘤患者,显示出良好的 耐受性及抗肿瘤活性[12]。在随机Ⅲ期 RADIANT-2 试验中,429 例晚期神经内分泌肿瘤和类癌综合 征患者随机接受长效奥曲肽联合依维莫司或安慰剂治疗[13],接受奥曲肽联合依维莫司治疗的患者 中位 PFS 为 16.4 个月,仅接受奥曲肽治疗的患者则为 11.3 个月,但两组 PFS 未达到统计学差异。RADIANT-4 是一项全球、双盲、安慰剂对照的Ⅲ期试验,入组 302 例进展期非功能性的肺或胃肠神 经内分泌肿瘤患者(其中肺神经内分泌肿瘤患者 90 例),以 2 :1 比例随机分配接受依维莫司或安慰
剂治疗[14],与安慰剂组相比(mPFS=3.6 个月),依维莫司组的中位无进展生存期(mPFS=9.2 个月)明显改善(HR 0.50;95%CI 0.28~0.88)[15]。依维莫司可推荐用于临床肿瘤负荷明显的低级别(类癌) 或疾病进展或中级别(不典型类癌)的局部晚期和 / 或远处转移支气管肺 / 胸腺神经内分泌肿瘤患者。
7. 放射性标记的生长抑素类似物治疗
一些早期研究报道,放射性标记的生长抑素类似物治疗对晚期神经内分泌肿瘤患者有效[16-20]。一项前瞻性Ⅱ期研究纳入 90 例对奥曲肽耐药的转移性神经内分泌肿瘤患者,结果显示放射肽治疗 可明显改善患者症状,但肿瘤退缩相对少见[21]。一些大型非随机队列分析也显示放射性标记的生长 抑素类似物治疗可改善患者生存率[22-24]。另一项最近的研究评估 177Lu-dotatate 在 610 例转移性胃肠 胰和肺神经内分泌肿瘤患者中的长期疗效、生存率和不良反应[25],所有患者的 PFS 和 OS 分别为 29 个月(95%CI 26~33 个月) 和 63 个月(95%CI 55~72 个月)[25]。2018 年 1 月,FDA 批准 177Lu- DOTATATE 的 PRRT 用于治疗不能切除、低或中度恶性,局部进展或转移性胃肠胰神经内分泌肿瘤[26]。NCCN 推荐对于某些胃肠道、支气管肺和胸腺神经内分泌肿瘤中生长抑素受体显像阳性的进展期和 / 或转移性胃肠道、支气管肺和胸腺神经内分泌肿瘤患者,可考虑使用 177Lu-dotatate 的肽受体放射性 核素治疗(PRRT) 作为治疗方案,鉴于目前国内尚未能开展该项治疗,仅作为Ⅲ级推荐。





参考文献
[1] CHONG C R, WIRTH L J, NISHINO M, et al. Chemotherapy for locally advanced and metastatic pul-monary carcinoid tumors [J] . Lung Cancer, 2014, 86(2): 241-246.
[2] WIRTH L J, CARTER M R, JANNE P A, et al. Outcome of patients with pulmonary carcinoid tumors receiving chemotherapy or chemoradiotherapy [J] . Lung Cancer, 2004, 44(2): 213-220.
[3] FILOSSO P L, YAO X, AHMAD U, et al. Outcome of primary neuroendocrine tumors of the thymus: a joint analysis of the International Thymic Malignancy Interest Group and the Euro- pean Society of Thoracic Surgeons databases [J] . J Thorac Cardiovasc Surg, 2015, 149(1): 103-109.
[4] RIMNER A, YAO X, HUANG J, et al. Postoperative radiation therapy is associated with longer overall survival in completely resected stageⅡ and Ⅲ thymoma-an analysis of the international thymic malignancies interest group retrospective database [J] . J Thorac Oncol, 2016, 11(10): 1785- 1792.
[5] BIAN D, QI M, HU J, et al. The comparison of predictive factors regarding prognoses and invasion of thymic neuroendocrine tumors preoperatively and postoperatively [J] . J Thorac Dis, 2018, 10(3): 1657- 1669.
[6] CRONA J, FANOLA I, LINDHOLM D P, et al. Effect of temozolomide in patients with metastatic bronchial carcinoids [J] . Neuroendocrinology, 2013, 98(2): 151-155.
[7] PAULSON A S, BERGSLAND E K. Systemic therapy for advanced carcinoid tumors: where do we go from here ?[J] J Natl Compr Canc Netw, 2012, 10(6): 785-793.
[8] MEDLEY L, MOREL A N, FARRUGIA D, et al. PhaseⅡ study of single agent capecitabine in the treatment of metastatic non-pancreatic neurondocrine tumours [J] . Br J Cancer, 2011, 104(7): 1067- 1070.
[9] BAJETTA E, CATENE L, Procopio G, et al. Are capecitabine and oxaliplatin (XELOX) suitable treat-ments for progressing low-grade and high-grade neuroendocrine tumours ?[J] Cancer Chemother Pharmacol, 2007, 59(5): 637-642.
[10] EKEBLA D S, SUNDIN A, JANSON E T, et al. Temozolomide as monotherapy is effective in treat-ment of advanced malignant neuroendocrine tumors [J] . Clin Cancer Res, 2007, 13 (10) : 2986-2991.
[11] CRONA J, FANOLA I, LINDHOLM DP, et al. Effect of temozolomide in patients with metastatic bronchial carcinoids [J] . Neuroendocrinology, 2013, 98(2): 151-155.
[12] YAO J C, PHAN A T, CHANG D Z, et al. Efficacy of RAD001 (everolimus) and octreotide LAR in advanced low-to intermediate-grade neuroendocrine tumors: results of a phase Ⅱ study [J] . J Clin Oncol, 2008, 26(26): 4311-4318.
[13] PAVEL M E, HAINSWORTH J D, BAUDIN E, et al. Everolimus plus octreotide long-acting repeat-able for the treatment of advanced neuroendocrine tumours associated with carcinoid syndrome (RADIANT-2) : a randomised, placebo-controlled, phase 3 study [J] . Lancet, 2011, 378(9808): 2005- 2012.
[14] YAO J C, FAZIO N, SINGH S, et al. Everolimus for the treatment of advanced, non-functional neu-roendocrine tumours of the lung or gastrointestinal tract (RADIANT-4) : a randomised, placebo- controlled, phase 3 study [J] . Lancet, 2016, 387(10022): 968-977.
[15] FAZIO N, BUZZONI R, DELLE F G, et al. Everolimus in advanced, progressive, well-differen-tiated, non-functional neuroendocrine tumors: RADIANT-4 lung subgroup analysis [J] . Cancer Sci, 2018, 109 (1): 174-181.
[16] IMHOF A, BRUNNER P, MARINCEK N, et al. Response, survival, and long term toxicity after therapy with the radiolabeled somatostatin analogue [90Y-DOTA] -TOC in metastasized neuroendo- crine cancers [J] . J Clin Oncol, 2011, 29(17): 2416-2423.
[17] KRENNING E P, TEUNISSEN J J, VALKEMA R, et al. Molecular radiotherapy with somatosta-tin analogs for (neuro-) endocrine tumors [J] . J Endocrinol Invest, 2005, 28(11 Suppl interna- tional): 146-150.
[18] KWEKKEBOOM D J, BAKKER W H, KAM B L, et al. Treatment of patients with gastro-entero-pancreatic (GEP) tumours with the novel radiolabeled somatostatin analogue [177Lu- DOTA(0), Tyr3] octreotate [J] . Eur J Nucl Med Mol Imaging, 2003, 30(3): 417-422.
[19] KWEKKEBOOM D J, TEUNISSEN J J, BAKKER W H, et al. Radiolabeled somatostatin ana-log [177Lu-DOTA0, Tyr3] octreotate in patients with endocrine gastro-enteropancreatic tumors [J] . J Clin Oncol, 2005, 23(12): 2754-2762.
[20] KWEKKEBOOM D J, TEUNISSEN J J, KAM BL, et al. Treatment of patients who have endocrine gastroenteropancreatic tumors with radiolabeled somatostatin analogues [J] . Hematol Oncol Clin North Am, 2007, 21(3): 561-573.
[21] BUSHNELL D L, O’DORISIO T M, O’DORISIO M S, et al. 90Y-edotreotide for metastatic carci-noid refractory to octreotide [J] . J Clin Oncol, 2010, 28(10): 1652-1659.
[22] KONG G, THOMPSON M, COLLINS M, et al. Assessment of predictors of response and long-term survival of patients with neuroendocrine tumour treated with peptide receptor chemoradionuclide therapy(PRCRT) [J] . Eur J Nucl Med Mol Imaging, 2014, 41(10): 1831-1844.
[23] VILLARD L, ROMER A, MARINCEK N, et al. Cohort study of somatostatin based radiopeptide therapy with [(90)Y-DOTA] -TOC versus [(90)Y-DOTA] -TOC plus [(177)Lu-DOTA] -TOC in neu- roendocrine cancers [J] . J Clin Oncol, 2012, 30(10): 1100-1106.
[24] HORSCH D, EZZIDDIN S, HAUG A, et al. Peptide receptor radionuclide therapy for neuroendo-crine tumors in Germany: first results of a multiinstitutional cancer registry [J] . Recent Results Can- cer Res, 2013, 194: 457-465.
[25] BRABANDER T, ZWAN WA, TEUNISSEN J J, et al. Long-Term efficacy, survival, and safety of [(177)Lu-DOTA(0), Tyr(3)] octreotate in patients with gastroenteropancreatic and bronchial neu- roendocrine tumors [J] . Clin Cancer Res, 2017, 23(16): 4617-4624.
[26] FDA approves new treatment for certain digestive tract cancers [news release] . Silver Springs, MD: US Food and Drug Administration; January 26, 2018.
[27] GRAND B, CAZES A, MORDANT P, et al. High grade neuroendocrine lung tumors: pathological characteristics, surgical management and prognostic implications [J] . Lung Cancer, 2013, 81(3): 404-409.
[28] SAJI H, TSUBOI M, MATSUBAYASHI J, et al. Clinical response of large cell neuroen-docrine carcinoma of the lung to perioperative adjuvant chemotherapy [J] . Anticancer Drugs, 2010, 21(1): 89-93.
[29] KENMOTSU H, NIHO S, ITO T, et al. A pilot study of adjuvant chemotherapy with iri- notecan and cisplatin for completely resected high-grade pulmonary neuroendocrine car- cinoma (large cell neuroendocrine carcinoma and small cell lung cancer) [J] . Lung Can- cer, 2014, 84(3): 254-258.
[30] GRIDELLI C, ROSSI A, AIROMA G, et al. Treatment of pulmonary neuro-endocrine tumours: state of the art and future developments [J] . Cancer Treatment Review, 2013, 39(5): 466-472.
[31] LO RUSSO G, PUSCEDDU S, PROTO C, et al. Treatment of lung large cell neuroendocrine carci- noma [J] . Tumour Biol, 2016, 37(6): 7047.
[32] DERKS J L, LEBLAY N, THUNNISESEN E, et al. Molecular subtypes of pulmonary large cell neuroendocrine carcinoma predict chemotherapy treatment outcome [J] . Clin Cancer Res, 2018, 24(1): 33.
[33] LEVRA M G, MAZIERES J, CA VALETT E, et al. Efficacy of immune checkpoint inhibitors in large cell neuroendocrine lung cancer: results from a French retrospective cohort [J] . Thoracic Oncol, 2017, 12: 707-712.
[34] WANG V E, URISMAN A, ALBACKERl L, et al. Checkpoint inhibitor is active against large cell neuroendocrine carcinoma with high tumor mutation burden [J] . J Immunotherapy of Can- cer, 2017, 5(1): 75.


【注释】
1. 转化性 SCLC 定义
在 NSCLC 疾病进程中,组织学类型可转化为 SCLC,统称为转化性 SCLC。转化性 SCLC 与经典的 SCLC 在病理形态、分子特征、临床表现及药物敏感性等方面具有相似性,但又不能完全被归类为经典 SCLC,也许可被归为一种新的 SCLC 亚型[1]。
2. 转化性 SCLC 的诊断必须进行肿瘤组织再次活检,病理学诊断仍是金标准。单靠基因特征和血浆检测仍无法可靠的判断患者是否发生了 SCLC 转化。
3. 转化性 SCLC 的发生机制尚未明确,目前存在以下几种假说。①肿瘤细胞异质性假说:基于穿刺活检等小标本的病理诊断具有局限性,不能全面反映肿瘤组织的整体情况,即有 NSCLC 和 SCLC 两种成分同时存在的可能性[2]。②肿瘤干细胞假说:携带敏感突变肿瘤细胞的肿瘤干细胞本身具有分化为神经内分泌肿瘤 细胞的潜能。在 TKIs 的暴露压力下,更易转化为 SCLC。③分子机制假说:在 TKIs 的治疗过程中, 出现了抑癌基因 RB1 和 TP53 的双重缺失突变,并在 SCLC 转化中扮演着重要角色[3]。
4. 转化性 SCLC 是 EGFR 突变患者耐药机制之一:转化性 SCLC 主要发生在携带 EGFR 敏感突变 经 EGFR TKI 治疗之后耐药的肺腺癌患者,发生率 5%~14%[4-8],一般发生在 TKIs 治疗后的 14~26 个 月[9]。大部分转化性 SCLC 保留了原有肺腺癌的基因突变(约占 83.3%)和 SCLC 的基因特征,如TP53 和 RB1 的缺失突变及 PIK3CA 突变等。患者一旦发生 SCLC 转化,疾病往往进展较快,总体 预后欠佳,中位生存期 6.0~10.9 个月[10,11]。
5. 转化性 SCLC 的治疗策略
目前尚缺乏前瞻性的随机对照研究,可根据 EGFR-TKI 治疗后进展模式选择相应治疗策略,对 于 EGFR TKI 耐药后出现系统性快速进展的转化性 SCLC,可选择标准的 SCLC 化疗方案;孤立病 灶进展的转化性 SCLC 可采用原 EGFR TKI/ 或标准的 SCLC 化疗方案联合局部治疗;系统性缓慢进 展的 SCLC 患者,可采用标准的 SCLC 化疗方案 ±EGFR TKI 治疗[12,13]。对于后两种情况的治疗推荐, 证据来源主要是案例报道及小样本的回顾性研究,最佳的治疗策略仍有待进一步研究。
参考文献
[1] NIEDERST M J, SEQUIST L V, POIRIER J T, et al. RB loss in resistant EGFR mutant lung adenocar- cinomas that transform to small-cell lung cancer [J] . Nat Commun, 2015, 6: 6377.
[2] Shao Y, Zhong D S. Histological transformation after acquired resistance to epidermal growth factor tyrosine kinase inhibitors [J] . Int J Clin Oncol, 2018, 23(2): 235-242.
[3] MARCOUX N, GETTINGER S N, O KANE G, et al. EGFR-mutant adenocarcinomas that trans- form to small-cell lung cancer and other neuroendocrine carcinomas: clinical outcomes [J] . J Clin Oncol, 2019, 37(4): 278-285.
[4] OSER M G, NIEDERST M J, SEQUIST L V, et al. Transformation from non-small-cell lung cancer to small-cell lung cancer: molecular drivers and cells of origin [J] . Lancet Oncol, 2015, 16(4): e165-e172.
[5] SEQUIST L V, WALTMAN B A, DIAS-SANTAGATA D, et al. Genotypic and histological evolution of lung cancers acquiring resistance to EGFR inhibitors [J] . Sci Transl Med, 2011, 3(75): 26r-75r.
[6] YU H A, ARCILA M E, REKHTMAN N, et al. Analysis of tumor specimens at the time of acquired resistance to EGFR-TKI therapy in 155 patients with EGFR-mutant lung cancers [J] . Clin Cancer Res, 2013, 19(8): 2240-2247.
[7] PIOTROWSKA Z, NIEDERST M J, KARLOVICH C A, et al. Heterogeneity underlies the emergence of EGFRT790 wild-type clones following treatment of T790M-positive cancers with a third-generation EGFR inhibitor [J] . Cancer Discov, 2015, 5(7): 713-722.
[8] LEE J K, LEE J, KIM S, et al. Clonal history and genetic predictors of transformation into small-cell carcinomas from lung adenocarcinomas [J] . J Clin Oncol, 2017, 35(26): 3065-3074.
[9] OSER MG, Niederse MJ, SWQUIST LV, et al. Transformation from non-small-cell lung cancer to small-cell lung cancer: molecular drivers and cells of origin [J] . Lancet Oncol, 2015, 16(4): e165- e172.
[10] MARCOUX N, GETTINGER S N, O’KANE G, et al. EGFR-mutant adenocarcinomas that trans-form to small-cell lung cancer and other neuroendocrine carcinomas: clinical outcomes [J] . J Clin Oncol, 2019, 37(4): 278-285.
[11] ROCA E, GURIZZAN C, AMOROSO V, et al. Outcome of patients with lung adenocarcinoma with transformation to small-cell lung cancer following tyrosine kinase inhibitors treatment: A systematic review and pooled analysis [J] . Cancer Treat Rev, 2017, 59: 117-122.
[12] TATEMATSU A, SHIMIZU J, MURAKAMI Y, et al. Epidermal growth factor receptor mutations in small cell lung cancer [J] . Clin Cancer Res, 2008, 14(19): 6092-6096.
[13] YANG J J, CHEN H J, YAN H H, et al. Clinical modes of EGFR tyrosine kinase inhibitor failure and subsequent management in advanced non-small cell lung cancer [J] . Lung Can- cer, 2013, 79(1): 33-39.





【注释】
1. 神经内分泌肿瘤的预后
支气管肺神经内分泌肿瘤的预后与分型、分期以及治疗情况都密切相关。国内统计数据显示 典型类癌手术切除后的预后良好,5 年生存率为 87%~100%;10 年生存率为 82%~87%,不典型类 癌的转移倾向和局部复发倾向相对较大,5 年生存率变化范围较广(30%~95%),10 年生存率为 35%~56%。LCNEC 患者的 1、3、5 年生存率分别为 56.4%、0%、0% 左右,这个结果与其他国内外 报告情况基本一致[7]。
2. 可切除肺 / 胸腺神经内分泌肿瘤
基于生长抑素受体的显像或 18F- 氟脱氧葡萄糖(FDG)PET-CT 扫描(对于高级别肿瘤) 通常不 推荐用于监测,但可用于评估病灶位置和肿瘤负荷,以便在随后可能复发的情况下进行比较,相关 的生化标记物评估包括嗜铬粒素 A 和 5-HIAA。
3. 局部晚期和 / 或远处转移性肺神经内分泌肿瘤
局部晚期和 / 或转移性神经内分泌肿瘤,或怀疑类癌综合征时,推荐进行包括胸部增强 CT 和 腹部 / 盆腔增强的多时相 CT 或 MRI,每 3~6 个月进行一次[8,9]。如果尚未进行生长抑素受体成像, 则建议评估肿瘤的生长抑素受体状态(如果考虑使用奥曲肽或兰瑞肽治疗)。分化差的支气管肺或胸 腺神经内分泌肿瘤对 68Ga-dotatate PET-CT 的亲和力差[10],故对分化差的神经内分泌肿瘤或不典型 类癌更推荐 PET-CT 检查。也可以考虑行嗜铬粒素 A 或 24 小时尿液或血浆 5-HIAA 生化标记物检测[11]。
如果怀疑存在类癌综合征,建议进行心脏病专科会诊和超声心动图检查,以评估患者是否患有类癌 性心脏病,并可考虑使用生长抑素受体成像来评估神经内分泌肿瘤的生长抑素受体状态。
参考文献
[1] MANAPOV F, KLOCKING S, NIYAZ M, et al. Timing of failure in limited disease (stage Ⅰ~Ⅲ) small-cell lung cancer patients treated with chemoradiotherapy: a retrospective analysis [J] . Tumori, 2013, 99 (6) : 656- 660.
[2] JOHNSON B E, LINNOILA R I, WILLIAMS J P, et al. Risk of second aerodigestive cancers increases in patients who survive free of small-cell lung cancer for more than 2 years [J] . J Clin Oncol, 1995, 13(1): 101-111.
[3] JOHNSON B E. Second lung cancers in patients after treatment for an initial lung cancer [J] . J Natl Cancer Inst, 1998, 90(18): 1335-1345.
[4] RICHARDSON G E, TUCKER M A, VENZON D J, et al. Smoking cessation after successful treatment of small-cell lung cancer is associated with fewer smoking-related second primary can- cers [J] . Ann Intern Med, 1993, 119(5): 383-390.
[5] KAWAHARA M, USHIJIMA S, KAMIMORI T, et al. Second primary tumours in more than 2-year disease-free survivors of small-cell lung cancer in Japan: the role of smoking cessation [J] . Br J Can- cer, 1998, 78(3): 409-412.
[6] PARSONS A, DALEY A, BEGH R, et al. Influence of smoking cessation after diagnosis of early stage lung cancer on prognosis: systematic review of observational studies with meta-analy- sis [J] . BMJ, 2010, 340: b5569.
[7] 李兆沛 , 孟祥文 , 宋伟 . 支气管肺神经内分泌肿瘤 140 例特征及预后分析 [J] . 河北医科大学学报 , 2012, 33(3): 304-305.
[8] CWIKLA J B, BUSCOMBE J R, CAPLIN M E, et al. Diagnostic imaging of carcinoid metastases to the abdomen and pelvis [J] . Med Sci Monit, 2004, 10(Suppl 3): 9-16.
[9] KALTSAS G, ROCKALL A, PAPADOGIAS D, et al. Recent advances in radiological and radionu-clide imaging and therapy of neuroendocrine tumours [J] . Eur J Endocrinol, 2004, 151(1): 15-27.
[10] KAYANI I, CONRY B G, GROVES A M, et al. A comparison of 68Ga-DOTATATE and 18F-FDG PET-CT in pulmonary neuroendocrine tumors [J] . J Nucl Med, 2009, 50(12): 1927-1932.
[11] FOX D J, KHATTAR R S. Carcinoid heart disease: presentation, diagnosis, and manage-ment [J] . Heart, 2004, 90(12): 1224-1228.
附表





肺神经内分泌肿瘤分类

病理诊断流程图

诊疗指南证据类别

推荐等级

人点赞

人收藏

打赏









 010-82736610
010-82736610
 股票代码: 872612
股票代码: 872612
 京公网安备 11010802020745号
京公网安备 11010802020745号











